What is it?
The World Health Organization (WHO) defines substance abuse as harmful or hazardous use of psychoactive substances, including alcohol and illicit drugs. Psychoactive substance use can lead to Substance Use Disorder — a cluster of behavioral, cognitive, and physiological phenomena that develop after repeated substance use, that typically include a strong desire to take the drug, difficulties in controlling its use, persisting in its use despite harmful consequences, a higher priority given to drug use than to other activities and obligations, increased tolerance, and sometimes a physical withdrawal state.[1]
Many factors determine whether someone will start to use or become dependent on drugs or alcohol. Risk factors can increase a person’s chances for abuse, while protective factors can reduce the risk. Risk factors for use among children and adolescents include unstable family relationships; exposure to physical, mental, and sexual abuse; mental illness, early aggressive behavior; poor social skills; poor academic performance; substance use among peers and family members; drug and alcohol availability; involvement with the juvenile justice system; drug experimentation; and poverty.[2, 3] Protective factors include parental monitoring; positive social relationships; academic competence; and anti-drug policies.
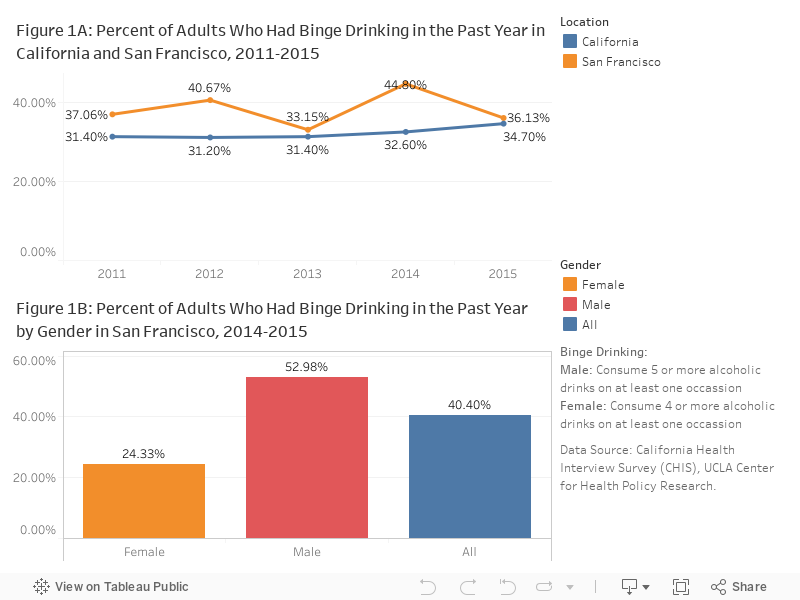
The negative effects of alcohol correlate with increased consumption. Moderate consumption is defined as having up to 1 drink per day for adult women and up to 2 drinks per day for adult men. Excessive alcohol consumption can refer to binge drinking, heavy drinking, drinking by persons under 21 years of age, and any alcohol use by pregnant women. Binge drinking is defined as any consumption leading to a blood alcohol concentration of 0.08% or more or about 4 drinks on a single occasion for adult women, or 5 drinks for adult men. Heavy drinking is defined as consumption of 8 or more drinks per week for women or 15 or more drinks per week for men.[4]
Why is it important for health?
The effects of drug and alcohol use are cumulative, and significantly contribute to costly social, physical, mental, and public health problems. These problems include poor academic performance, cognitive functioning deficits, unintended pregnancy, HIV and other sexually transmitted diseases, motor vehicle crashes, violence, child abuse, crime, homicide, chronic diseases including liver disease and certain cancers (e.g. colorectal, liver, breast, prostate), and mental and behavioral disorders (unipolar depressive disorders, epilepsy, suicide).[5] Unintentional poisoning is now the leading cause of injury death among American adults, surpassing motor vehicle accidents. In 2016, more than 64,000 deaths occurred due to drug overdoses, primarily from heroin and other natural and synthetic opioids.[6] Approximately 88,000 deaths result from alcohol use annually in the U.S. and in 2012 more than 10,000 persons died in alcohol-related motor vehicle accidents alone.[7,8]
Drug and alcohol use are both causes and effects of violence. More than half of all persons arrested for major crimes including homicide and assault were under the influence of drugs at the time of their arrest and over 42 percent of violent crimes reported to the police involved alcohol.[9,10] More than half of all substantiated cases of child abuse and neglect involve substance abuse.[11] Those who experience violence are also more likely to abuse drugs and alcohol. Women who have experienced childhood abuse or neglect are more likely to have problems with alcohol and over two-thirds of patients in drug abuse treatment centers report having been physically or sexually abused as children.[9,12]
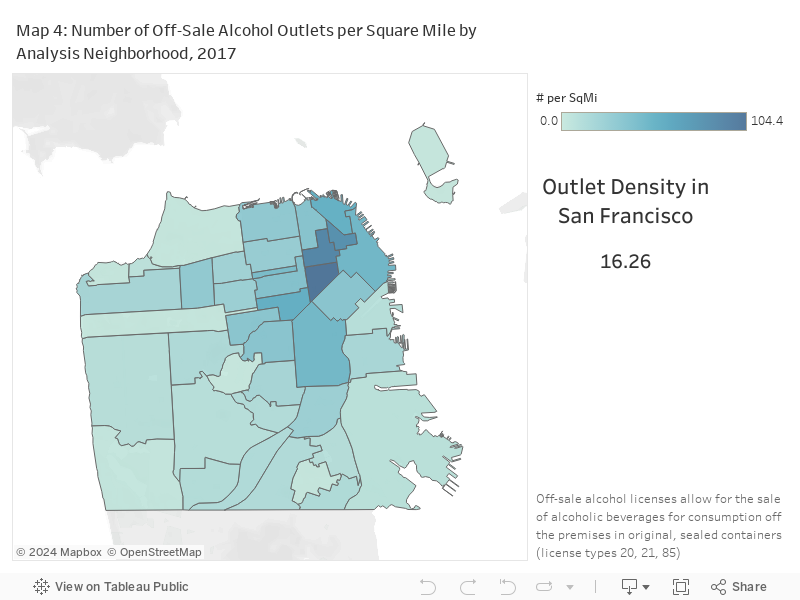
Research suggests that geographic density of alcohol outlets is closely related to crime and violence.[13] One study in New Jersey, controlled for age and poverty, found that neighborhoods with higher densities of alcohol outlets had more violent crimes, including homicide, rape, assault, and robbery.[14] In Los Angeles, a higher density of alcohol outlets was associated with more violence, after controlling for unemployment, age, ethnic and racial characteristics, and other community characteristics.[15] In a six-year study of alcohol outlets in 551 urban and rural zip code areas in California, an increase in the number of bars and off-premise establishments (e.g. liquor, convenience, and grocery stores) was correlated to an increase in the rate of violence.[16] These effects were largest in poor, minority areas of the state, already saturated with the greatest numbers of outlets.
Drug and alcohol have lasting impacts on children exposed intrauterine. Drug use during pregnancy can lead to premature birth, low birth weight, cognitive problems, and substance dependence in the baby.[17] Alcohol use during pregnancy causes fetal alcohol syndrome which includes mental retardation, malformation of the skeleton, heart and brain, and other developmental complications.[18] Children with prenatal exposure to drugs and alcohol are more likely to need special education services in school.
The earlier a person begins to use drugs and alcohol, the more likely he or she is to develop serious problems. The adolescent brain is negatively affected by alcohol and other drugs (e.g., cannabis) through altered function of neurotransmitters, altered perception, and habits and choices associated with drug and alcohol use becoming ingrained.[19] Adolescents exposed to drugs and alcohol before age 15 are more likely to be dependent as adults, to contract a herpes infection, to become pregnant as an adolescent, and to be involved in crime.[20]
Drug and alcohol abuse put the user at increased risk for communicable and chronic diseases. In 2000, one third of AIDS cases in the US resulted from injection drug use; about half of pediatric AIDS cases resulted from injection drug use or sex with an injection drug user by the mother.[21] Nearly all hepatitis C cases are attributable to injection drug use.[22] Alcohol consumption can also lead to high blood pressure, various cancers, heart disease, stroke, and liver disease.[23] Alcohol use has been estimated to cause 3.5% of cancer deaths in the US, with each deaths associated with 17 to 19 years of life lost.[24]
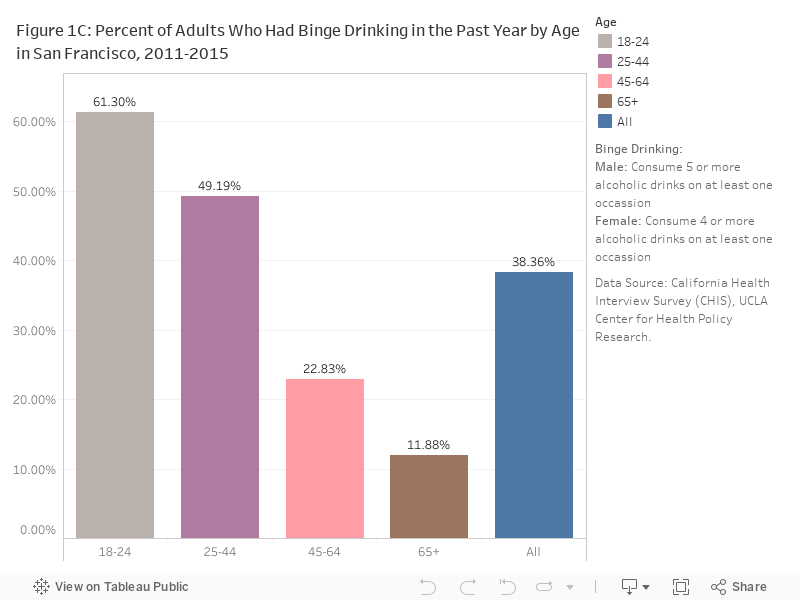
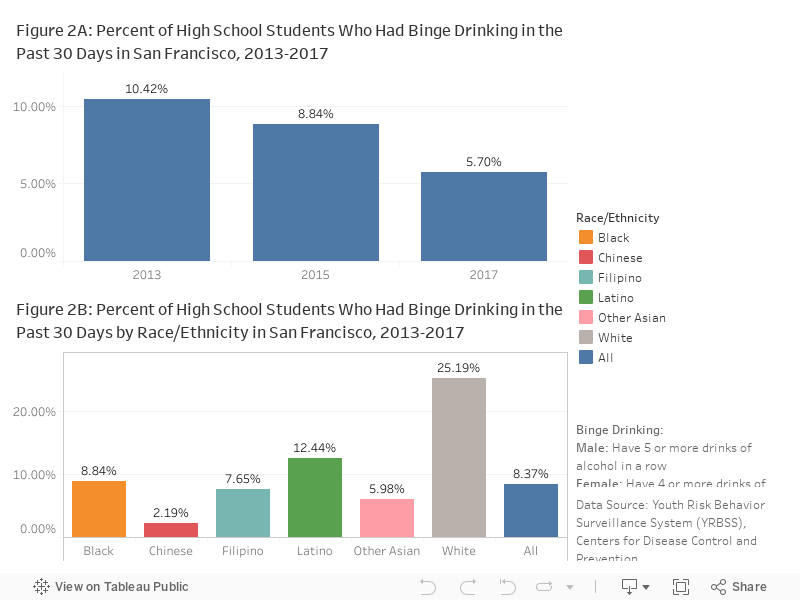
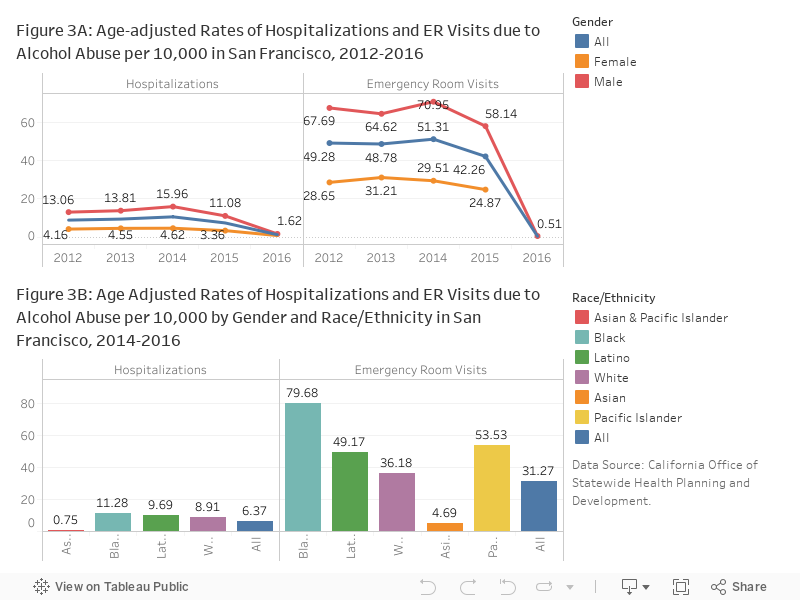
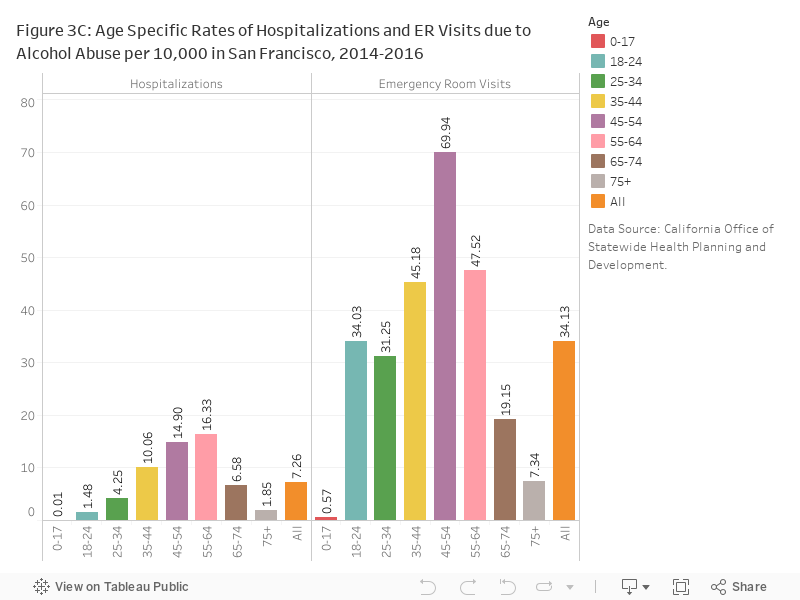
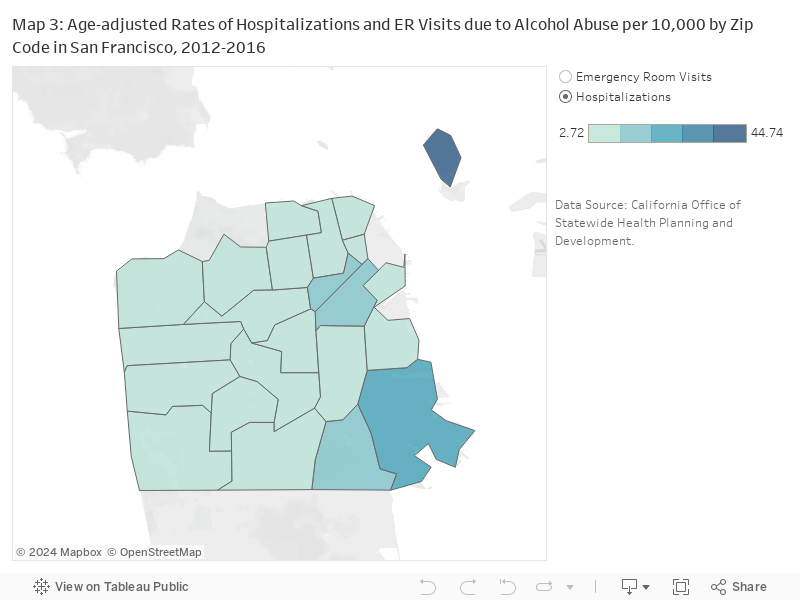
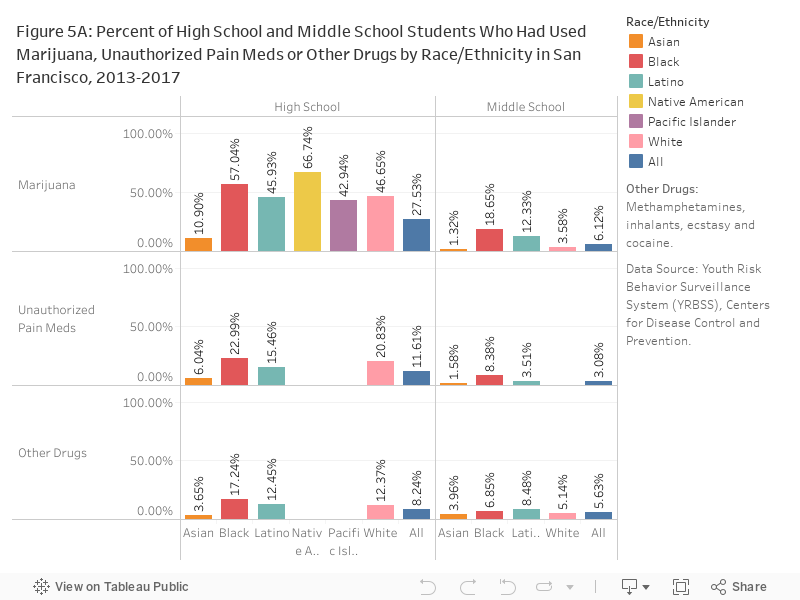
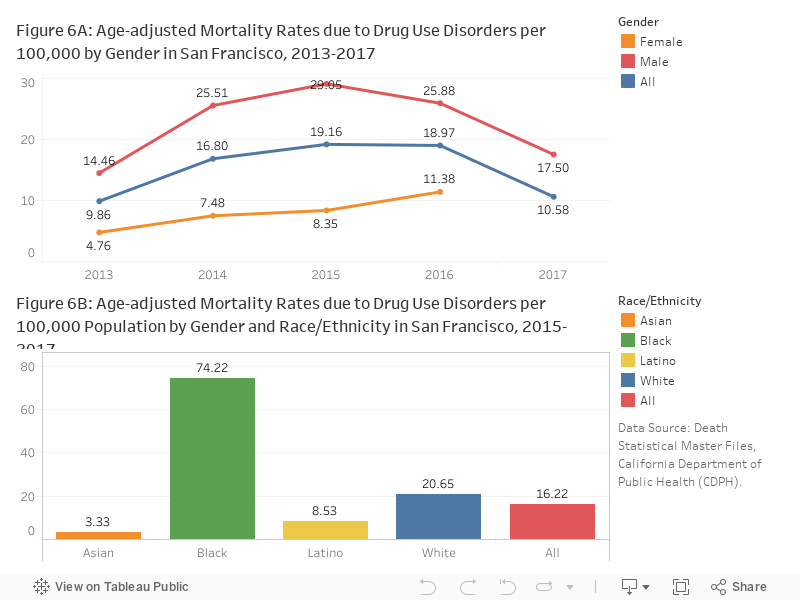
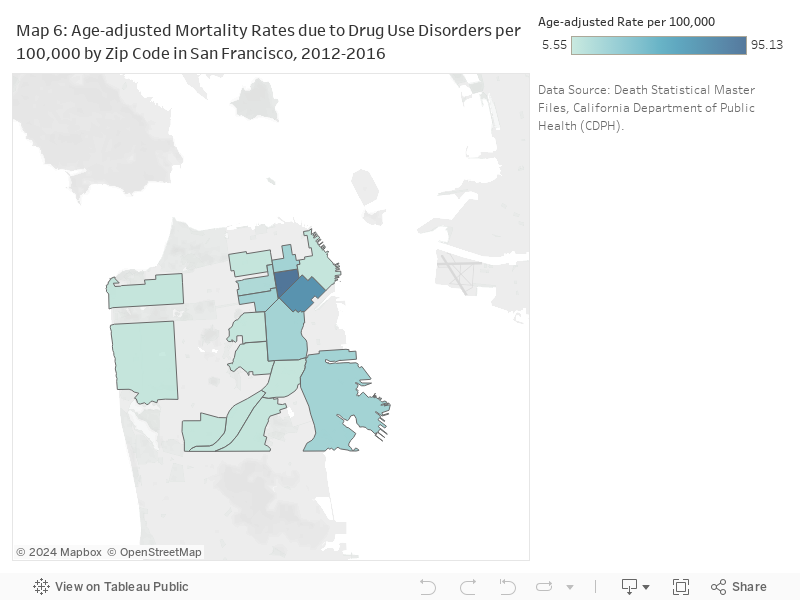
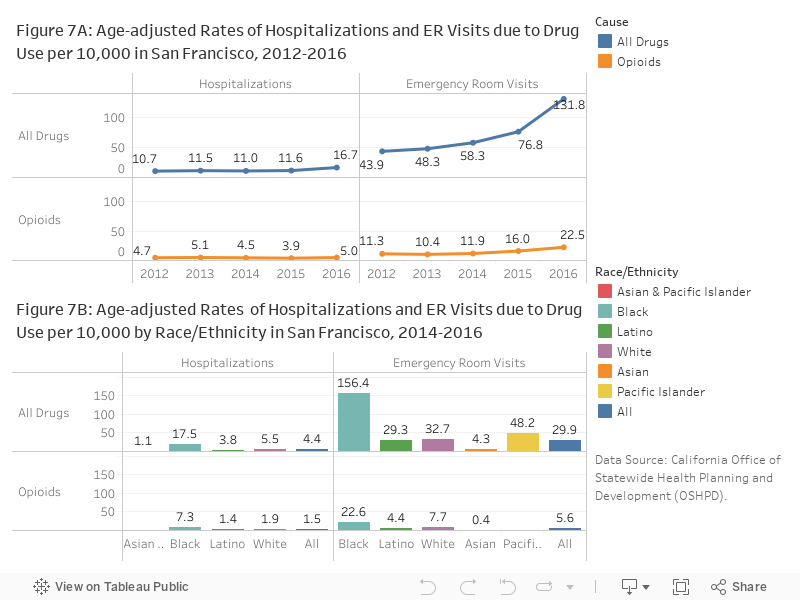
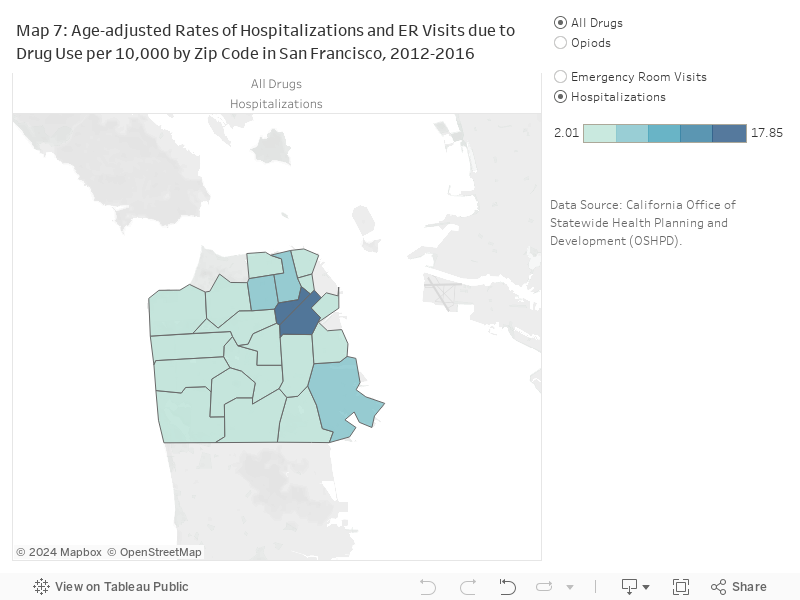
What is the status in San Francisco?