Variables
- LIVE BIRTHS THAT OCCURRED BEFORE 37 COMPLETED WEEKS OF GESTATION
- LIVE BIRTHS THAT OCCURRED BEFORE 32 COMPLETED WEEKS OF GESTATION
Preterm birth is the birth of an infant before 37 completed weeks of pregnancy. Births that occur before 32 weeks of pregnancy are considered very preterm, and are at highest risk for morbidity and mortality.[1] The national Healthy People (HP) 2020 objectives are to reduce all preterm births to no more than 9.4 percent of live births, reduce late preterm births (at 34 to 36 weeks of gestation) to 6.8 percent, reduce births at 32 to 33 weeks of gestation to 1.1 percent, and reduce very preterm births to no more than 1.5 percent of live births.[2]
Nationally, preterm birth rates vary by race-ethnicity. Black/African American women have the highest rates of preterm birth, approximately 1.5 times the rate seen in all other women.[3,4] In 2016, California ranked #22 among states in terms of race-ethnic preterm birth disparities.[4]
At the neighborhood level, preterm birth is associated with poverty, low educational attainment, pollution, residential segregation, crime rates, gentrification and housing instability.[1,5,6] At the individual level, during pregnancy, experience of racism and poverty, stress or anxiety, lack of support, substance use (tobacco, alcohol, or cocaine), and delayed or inadequate prenatal care are associated with increased risk of preterm birth.[1,7]
Prematurity is the leading cause of infant mortality in the United States.[1] A developing baby goes through important growth during the last weeks and months of pregnancy. Many organs, including the brain, eyes, lungs, and liver, need the final weeks of pregnancy to fully develop. Preterm infants often face a lifetime of disability, including learning disabilities and visual, hearing, and neurological problems.[8] Being born premature may also negatively affect a person’s social-emotional development.[1] Furthermore, because the risk of preterm birth is determined by the accumulation of exposures over a woman’s lifetime and a preterm birth can affect a person’s health throughout the life course, preterm birth rates are often used as a measure of overall population health.[9]
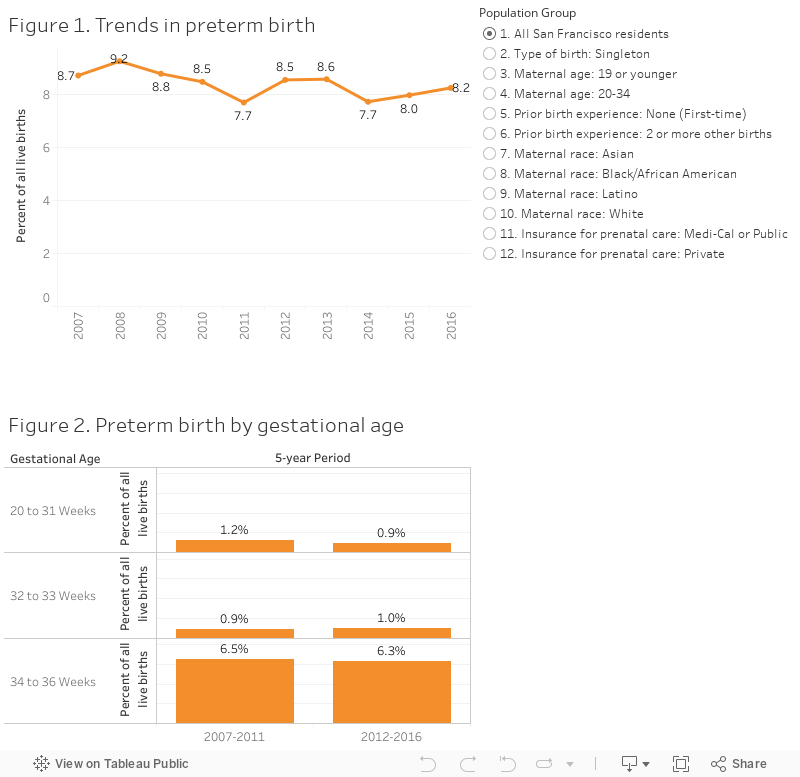
In 2016, 8.2 percent of live births to San Francisco residents were preterm. Fewer than 1 percent of births (86 births) were very preterm. The citywide preterm birth rate did not change significantly between 2012-2016.
Over the five year period, 6.3 percent of births occurred at 34 to 36 weeks gestation, 1.0 percent of births occurred at 32 to 33 weeks gestation, and 0.9 percent of births were born before 32 weeks gestation (See Figures 1, 2).
Although San Francisco has met national HP 2020 targets for risk of preterm birth, at the citywide level, elevated risk of preterm birth persists for vulnerable population groups. Consistent with national patterns, elevated risk of preterm birth is associated with neighborhood and living conditions, demographic and socio-economic variables, smoking status, and adequacy of prenatal care (See Figures A-H).
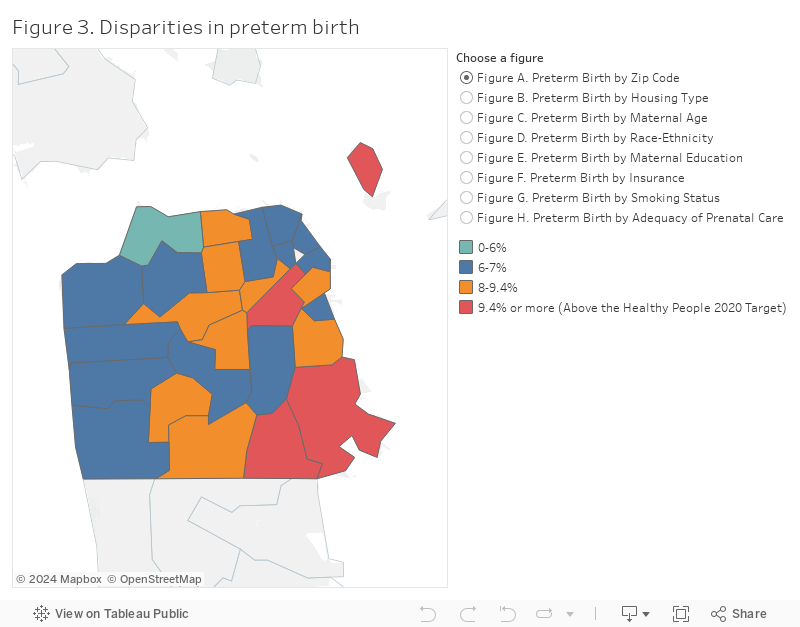
In 2012-2016, 11.0 percent of births in the Bayview zip code 94124 were born preterm. Over 10 percent of live births for women with no address (homeless), an address at a single resident occupancy (SRO) hotel, or an address in public housing were preterm. Whereas 7.3 percent of White births were preterm, 13.8 percent of Black/African American births were preterm. Among women with less than a high school education, 9.8 percent of births were preterm. Among women with no health insurance coverage for prenatal care, 41.0 percent of births were preterm. Smoking in the 3 months before pregnancy doubled the risk of preterm birth from 8.4 percent to 15.4 percent. 17.6 percent of births to women with unknown prenatal care were preterm.
Many programs in San Francisco are working towards reducing rates of preterm birth. The Department of Public Health, Black Infant Health, Public Health Nursing, Comprehensive Perinatal Services Program (CPSP), Women Infant and Children (WIC) program, and Project 500 are providing various kinds of support for women most at risk of preterm birth. UCSF’s Preterm Birth Initiative supports a wide variety of research aimed at reducing the incidence and burden of preterm birth. Some community-based organizations like Homeless Prenatal are working hard to address some of the social determinants of preterm birth with at-risk San Franciscans. Collaborations such as the San Francisco Collective Impact to Prevent Preterm Birth, Solid Start, and the Joint Perinatal Health Equity Project, have also set out to address some of the determinants of preterm birth by bringing together key stakeholders from a variety of organizations to coordinate their efforts and maximize their resources. Led by the community-based doula program, SisterWeb, the city will be supporting the development of a doula program geared to provide culturally relevant doula services for families at highest risk for maternal mortality and premature birth, an intervention proven to be effective in improving birth outcomes. [13]
There is limited evidence for interventions which produce population-level decreases in preterm birth rates. Preterm birth rates may be improved by interventions that can reduce stress on girls and women, especially those from the communities most impacted.[1] Programs which improve social support for the women most at risk are likely to positively impact preterm birth rates.[10] Increasing the cultural competence and racial diversity of medical providers and expanding availability of community-based health workers and doulas are key strategies to address racial disparities in birth outcomes.[10,11] Policies that decrease poverty, increase educational opportunities, improve housing quality and stability, and increase health care access within African American communities have potential for reducing San Francisco’s preterm birth rate.[11]
California Department of Public Health. Birth Statistical Master File.
Preterm and very preterm birth were defined in terms of the best obstetric estimates of gestational age, determined by ultrasound measurements of the embryo or fetus during the first trimester of pregnancy. This methodology is consistent with Centers for Disease Control, American Congress of Obstetricians and Gynecologists, and California Department of Public Health protocol.[12]
The validity of the preterm birth estimates depends on the quality of data collected on birth records, which is known to vary from hospital to hospital.
[1] Butler AS, Behrman RE, et al. Preterm birth: causes, consequences, and prevention. National Academies Press, 2007.
[2] Healthy People 2020. Maternal, infant, and child health overview. https://www.healthypeople.gov/2020/topics-objectives/topic/maternal-infant-and-child-health/objectives, 2017.
[3] Centers for Disease Control and Prevention. Reproductive health, Preterm birth. https://www.cdc.gov/reproductivehealth/MaternalInfantHealth/PretermBirth.htm
[4] March of Dimes. 2016 Premature birth report card. https://www.marchofdimes.org/materials/premature-birth-report-card-united-states.pdf
[5] Huynh M, Maroko AR. Gentrification and preterm birth in New York City, 2008–2010. Journal of Urban Health, 91(1):211–220, 2014.
[6] Kane JB, Miles G, Yourkavitch J, King K. Neighborhood context and birth outcomes: Going beyond neighborhood disadvantage, incorporating affluence. SSM Population Health 2017; 3: 699-712.
[7] Braveman P, Heck K, Egerter S, Dominguez TP, Rinki C, Marchi KS, Curtis M. Worry about racial discrimination: A missing piece of the puzzle of Black-White disparities in preterm birth? Plos One 2017; 12(10): e0186151.
[8] State Infant Mortality Collaborative: Infant Mortality Toolkit. State infant mortality (sim) toolkit: A standardized approach for examining infant mortality. http://www.amchp.org/programsandtopics/data-assessment/InfantMortalityToolkit/Pages/default.aspx, November 2013.
[9] Lu MC, Kotelchuck M, Hogan V, Jones L, Wright K, Halfon N. Closing the black-white gap in birth outcomes: A life-course approach. Ethnicity & disease, 20(1 0 2):S2, 2010.
[10] Gruber KJ, Cupito SH, Dobson CF. Impact of doulas on healthy birth outcomes. The Journal of perinatal education, 22(1):49, 2013.
[11] Centers for Disease Control and Prevention. CDC Health disparities and inequalities report: United states. https://www.cdc.gov/minorityhealth/chdireport.html, 2013.
[12] Healthy People 2020. Preterm births and infant deaths. https://www.healthypeople.gov/2020/leading-health-indicators/infographic/maternal-infant-and-child-health-0, 2017.
[13] Gruber, K. J., Cupito, S. H., & Dobson, C. F. (2013). Impact of Doulas on Healthy Birth Outcomes. The Journal of Perinatal Education, 22(1), 49–58. http://doi.org/10.1891/1058-1243.22.1.49
