What is currently being done in San Francisco to improve oral health?
Beginning in 2012, a citywide collaborative, now known as CavityFreeSF, formed to reduce children’s caries experience and disparities. CavityFreeSF developed the San Francisco Children’s Oral Health Strategic Plan 2014-2017, which aimed to “increase awareness and practice of optimal children’s oral health behaviors among diverse communities”, “increase access to oral health services”, and “integrate oral health with overall health.” [27]
Implementation of the strategic plan resulted in 16 additional medical clinics, in 3 large medical systems, providing fluoride varnish applications at pediatric well-child visits for children under age 6. In 2016, fluoride varnish applications were administered to 1,752 children through primary care clinics. [28]
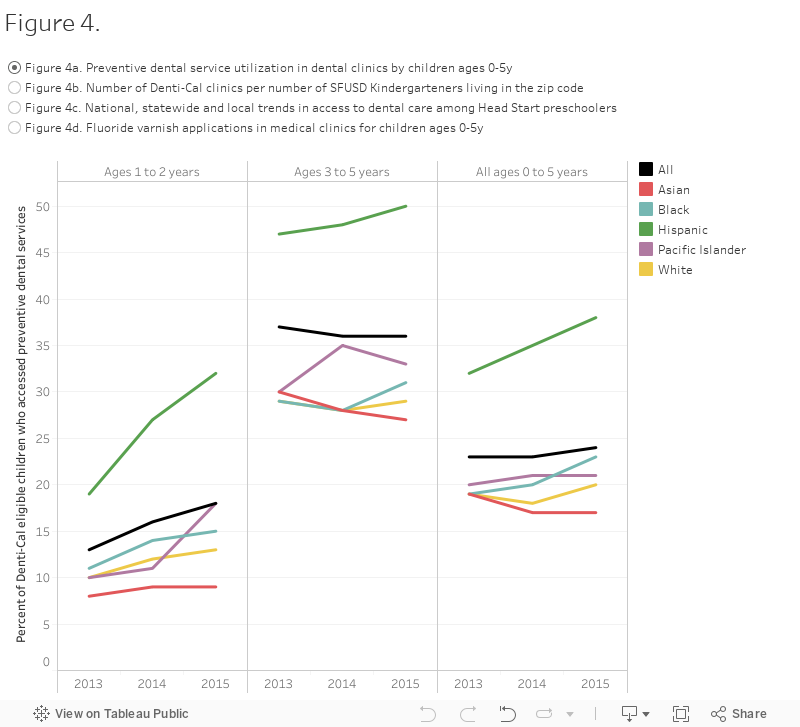
With funding from California Department of Public Health (CDPH)-Oral Health Program, California Department of Health Care Services (DHCS) Prop 56, and Dental Transformation Initiative and in collaboration with Our Children Our Families, CavityFree SF aims to reduce caries experience from 39 to 27 percent; reduce untreated decay from 18 to 8 percent by 2020; reduce the difference in caries experience between Asian, Black, and Hispanic/Latino kindergarteners and White kindergarteners from 20 to 15 percentage points; reduce the race-ethnic disparity in untreated decay from 8 to 6 percentage points; and increase the percentage of Denti-Cal eligible children who have seen a dental provider by age 2 from 27 to 31 percent, all by 2020. San Francisco Dental Transformation Initiative Local Dental Pilot Program, working with CavityFreeSF, will implement 5 pilot projects to increase access to dental services, increase dental care coordination, develop health promotion messages, increase interprofessional collaboration, and incentivize FQHC dual-users. [29-32]
Data Sources
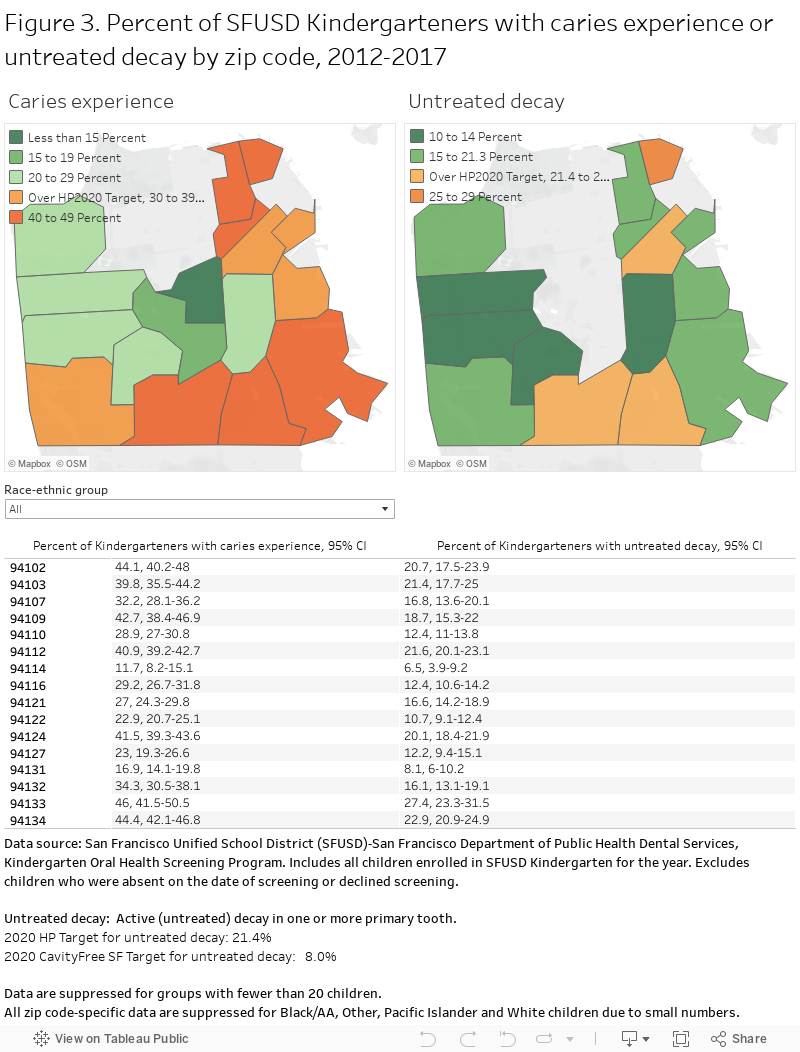
1. San Francisco Unified School District (SFUSD)-San Francisco Department of Public Health (SFDPH) Dental Services. Kindergarten Oral Health Screening Program.
2. California Department of Health Care Services (DHCS), Medi-Cal Management Information System/Decision Support System, 2012.
3. Head Start PIR (Program Information Report) data 2008 to 2016.
4. CHDP Children’s Dental Referral Directory available at https://www.sfhp.org/programs/medi-cal/benefits/dental-services/
5. San Francisco Department of Public Health, San Francisco Denti-Cal Clinic Capacity Survey.
6. San Francisco Health Network program data, Fluoride Varnish Applications for Children Age 0-5 Years, 2014-2018.
Methods and Limitations
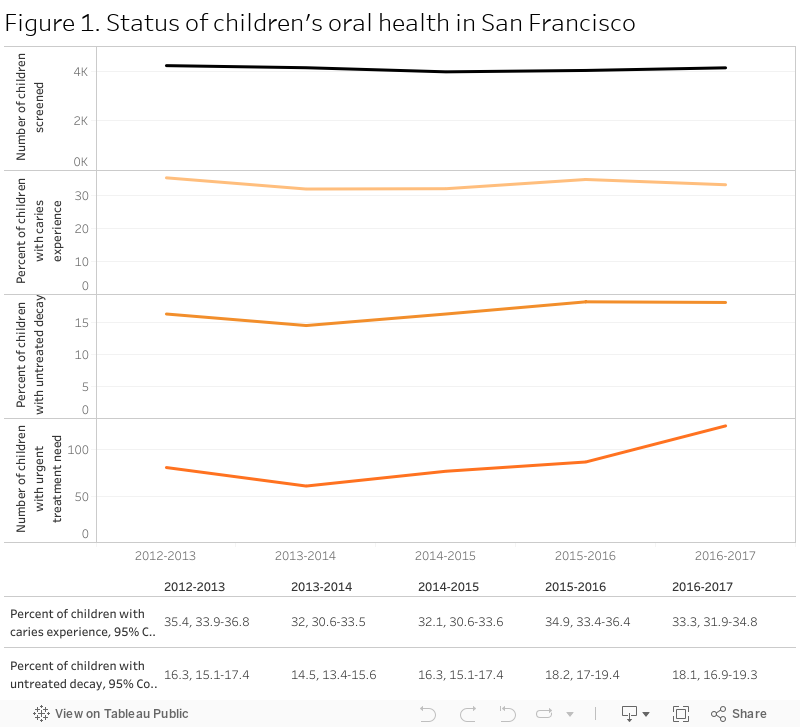
Caries experience is defined as having one or more untreated or treated (filled) cavity. Low income is defined at or below 200 percent of the Federal Poverty Level.
Between 2007–08 and 2016–17, the SFDPH Dental Services offered annual oral health screening to all children enrolled in kindergarten classes in the San Francisco Unified School District, excluding children in charter schools. Approximately 4,000 children were screened each year. Families were notified of the date of the oral health screening by flyer and a note sent home with each child. Children who were absent or who did not assent to screening on the date specified were not screened.
Forty to fifty licensed, volunteer dentists from the San Francisco Dental Society (SFDS) conducted the dental screenings. The program annually gave the dentists a written training module detailing the clinical data to collect and the diagnostic criteria to use. The oral health information collected for each child included the number of primary and permanent teeth with untreated or treated decay and treatment need. The diagnostic criteria defined treatment need in terms of Class I, Class II, and Class III categories:
Class I: No visible dental problems. Individuals apparently require no dental treatment.
Class II: Mild dental problems. Individuals require treatment, but not of an urgent nature. Class II problems include pinhead-size cavities that are not generalized or advanced, moderate plaque and calculus accumulation indicating the need for oral prophylaxis, or other oral conditions requiring corrective or preventive measures.
Class III: Severe or emergency dental problems. Individuals require treatment of cavities as large as a green pea, extensive pinhead cavities, chronic abscess(es), acute or chronic oral infection, heavy calculus accumulation, insufficient number of teeth for mastication, injuries, and/or painful conditions.
The San Francisco indicator may underestimate the prevalence of caries experience. To allow comparison of local data with national caries experience estimates, the San Francisco indicator does not include extracted teeth or count caries in permanent teeth. The HP 2020 target focuses on caries experience in primary teeth. The National Health and Nutrition Examination Survey does not capture data on extracted or missing primary teeth.
References
[1] World Health Organization (WHO). Oral health fact sheet. http://www.who.int/oral_health/publications/factsheet/en/
[2] Centers for Disease Control and Prevention (CDC). Children’s Oral Health.
https://www.cdc.gov/oralhealth/children_adults/child.htm
[3] Mommy It Hurts to Chew The California Smile Survey. (2006, February). Retrieved from https://centerfororalhealth.org/wp-content/uploads/2018/02/Mommy-It-Hurts-To-Chew.compressed.pdf
[4] American Dental Association. ADA policy-Definition of oral health. https://www.ada.org/en/about-the-ada/ada-positions-policies-and-statements/ada-policy-definition-of-oral-health
[5] American Dental Association. Oral health. https://www.mouthhealthy.org/en/az-topics/o/oral-health
[6] Marinho VCC, Worthington HV, Walsh T, Clarkson JE. Fluoride varnishes for preventing dental caries in children and adolescents. Cochrane Database of Systematic Reviews. 2013; Issue 7. Art. No.: CD002279. DOI: 10.1002/14651858.CD002279.pub2.
[7] Chazin Z, Glover J. A Community Framework for Addressing Social Determinants of Oral Health for Low-Income Populations. Center for Health Care Strategies. Technical Assistance Brief, January 2017. https://www.chcs.org/media/SDOH-OH-TA-Brief_012517.pdf
[8] Capizzano J, Adams G. The hours that children under five spend in child care: variation across states. https://www.urban.org/sites/default/files/publication/62106/309439-The-Hours-That-Children-Under-Five-Spend-in-Child-Care.PDF
[9] Benjamin R. Oral health: the silent epidemic. Public Health Rep 2010; 125(2): 158-159.
[10] Oral Health Child Health and Disability Prevention Program, Health Assessment Guidelines
California Department of Health Care Services, Systems of Care Division. (2016,March).
http://www.dhcs.ca.gov/services/chdp/Documents/HAG/18OralHealth.pdf
[11] Children with dental caries experience in their primary teeth (percent, 3–5 years). (n.d.). https://www.healthypeople.gov/2020/data/Chart/4992?category=1&by=Total&fips=-1
[12] Heathy People 2020. Oh-1.2 reduce the proportion of children aged 6 to 9 years with dental caries experience in their primary or permanent teeth. https://www.healthypeople.gov/2020/data/Chart/4993?category=1&by=Total&fips=-1
[13] Pourat, Nadereh & Nicholson, Gina. (2009). Unaffordable dental care is linked to frequent school absences. Policy brief (UCLA Center for Health Policy Research). 1-6.
[14] Gupta N, Vujicic M, Yarbrough C, Harrison B. Disparities in untreated caries among children and adults in the U.S., 2011–2014. BMC Oral Health. 2018; 18: 30. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5840689/
[15] Oral Health – Health people 2020. (n.d.). Retrieved from https://www.healthypeople.gov/2020/topics-objectives/topic/oral-health/objectives
[16] https://www.cda.org/Portals/0/pdfs/untreated_disease.pdf
[17] Jackson SL, Vann WF, Kotch JB, Pahel BT, Lee JY. Impact of Poor Oral Health on Children’s School Attendance and Performance. American Journal of Public Health. 2011;101(10):1900-1906. doi:10.2105/AJPH.2010.200915.
[18] Seirawan, H., Faust, S and Mulligan, R.(2012, September). “The impact of oral health on the academic performance of disadvantaged children.” Am J Public Health.;102(9):1729-34. doi: 10.2105 /AJPH.2011. 300478. Epub 2012 Jul 19.5.
[19] Cordeiro MM, Rocha MJ. The effects of periradicular inflammation and infection on a primary tooth and permanent successor. J Clin Pediatr Dent. 2005 Spring;29(3):193-200.
[20] Cardoso EM, Reis C, Manzanares-Céspedes MC. Chronic periodontitis, inflammatory cytokines, and interrelationship with other chronic diseases. Postgrad Med. 2018 Jan;130(1):98-104. doi: 10.1080/00325481.2018.1396876. Epub 2017 Nov 8.
[21] Giannopoulou C, Cionca N, Almaghlouth A, Cancela J, Courvoisier DS, Mombelli A. Systemic Biomarkers in 2-Phase Antibiotic Periodontal Treatment: A Randomized Clinical Trial. J Dent Res. 2016 Mar;95(3):349-55. doi: 10.1177/0022034515618949. Epub 2015 Nov 24.
[22] Cholera M, Fisher M, Stookey J, San Francisco Department of Public Health. Capacity of Dental Clinics in San Francisco to Serve Children Ages 0-5 years With Denti-Cal Insurance in Summer 2018: A Cross sectional survey. Slide presentation available at https://www.sfdph.org/dph/comupg/oprograms/MCH/Epi.asp
[23] Gupta N, Yarbrough C, Vujicic M, Blatz A, Harrison B. Medicaid fee-for-service reimbursement rates for child and adult dental care services for all states, 2016. Health Policy Institute Research Brief. American
[24] https://www.cda.org/news-events/rate-increases-and-benefit-restoration-for-denti-cal-program
[25] Head Start: Background and Funding. (2014, January 2) Retrieved from https://www.everycrsreport.com/files/20140102_RL30952_9de5df5a6c4debc9131eea76fb96ade27155c351.pdf
[26] “Head Start Timeline.” ECLKC. N.p., 01 Apr. 2018. https://eclkc.ohs.acf.hhs.gov/about-us/news/head-start-timeline
[27] San Francisco Children’s Oral Health Strategic Plan 2014-2017. (2014, November). Retrieved from http://assets.thehcn.net/content/sites/sanfrancisco/Final_document_Nov_2014_20141126111021.pdf
[28] Stookey, J. D., Et al. (2017, August 8). Case Study: School-Based Oral Health Screening in San Francisco as an Essential Public Health Service. Retrieved from https://www.sfdph.org/dph/files/MCHdocs/Epi/Journal-Article-School-Based-Oral-Health-Screening-in-San-Francisco-as-an-Essential-Public-Health-Service-2017.pdf
[29] CDPH – Oral Health Program – Proposition 56 Local Oral Health Program OVERVIEW. (2017, July 26). Retrieved from http://cheac.org/wp-content/uploads/2017/07/LHJ-Informational-Webinar.pdf
[30] SF Dental Transformation Initiative – https://sfdti.weebly.com/
[31] “Home.” Our Children Our Families Council of San Francisco, Council San Francisco, https://www.ourchildrenourfamilies.org/
[32] CavityFree SF – San Francisco Children’s Oral Health Strategic Plan (2018, January). Retrieved from https://sfhip.org/content/sites/sanfrancisco/San_Francisco_Childrens_Oral_Health_Strategic_Plan_2014-2020.pdf