Variables
- High Blood Pressure among Adults
- Hospitalization due to Hypertension
- Heart Disease among Adults
- Hospitalization due to Heart Failure
- Medicare Beneficiaries Treated for Stroke
According to the American Heart Association, cardiovascular disease refers to a class of diseases that involves the heart and blood vessels. Many of these diseases are attributed to atherosclerosis, a condition where excess plaque builds up in the inner walls of the arteries. This buildup narrows the arteries and constricts blood flow. Hypertension, also called high blood pressure, is a condition where the force of blood pushing against the vessel walls is higher than normal [1]. Listed below are some common types of cardiovascular disease:
Cardiovascular disease and stroke are largely preventable yet heart disease and stroke remain the first and third leading causes of death in the United States, respectively [3]. Eighty percent of deaths due to ischemic heart disease and 50% of deaths due to stroke result from preventable factors including obesity, poor physical activity, drinking alcohol, smoking cigarettes, eating unhealthy foods (especially foods with added sugar), and not controlling blood pressure and cholesterol levels [4]. Conversely, eating well, being physically active, and avoiding alcohol and tobacco protect against cardiovascular disease and stroke. Whether or not someone is able to or desires to adopt healthy behaviors is impacted by institutional policies and practices, and living conditions, especially physical and social environments, which interact to promote or inhibit behaviors. Additional information on nutrition, physical activity, tobacco use, alcohol use, and weight is available in their respective sections of this assessment.
People with metabolic disease and/or diabetes are at increased risk for cardiovascular disease and stroke. Someone has metabolic disease if they have at least three of the following metabolic risk factors: a large waistline, high triglyceride levels, low HDL cholesterol level, high blood pressure, and high fasting blood sugar [5-6]. Adults with diabetes are two to four times more likely to die from heart disease than adults without diabetes [7]. It is possible to prevent, delay or improve metabolic disease, diabetes, and subsequent cardiovascular disease through lifestyle changes.
Black/African Americans, Native Americans and Latinos have higher rates of cardiovascular disease and associated risk factors [8]. Black/ African Americans are 30% more likely to die from heart disease and two time more likely to have a stroke [9]. Native Americans are twice as likely to die of cardiovascular disease before the age of 65 compared to all Americans [10]. Black/African Americans, Mexican Americans, and Native Americans are more likely to have risk factors associated with cardiovascular disease including high blood pressure, obesity, and diabetes, as well as are more likely to lack access to quality medical care and to live in high stress, low opportunity environments than are Whites [9, 11-14]. While risk factors for cardiovascular disease among Asian and Pacific Islanders overall appear to be similar to those of Whites, there is wide variation across Asian and Pacific Islander subgroups. For example, Korean, Vietnamese, and Filipino men have some of the highest smoking rates in the US and the prevalence of type 2 diabetes is more than twice as high for Asian Indians compared to Chinese or Japanese [14-15].
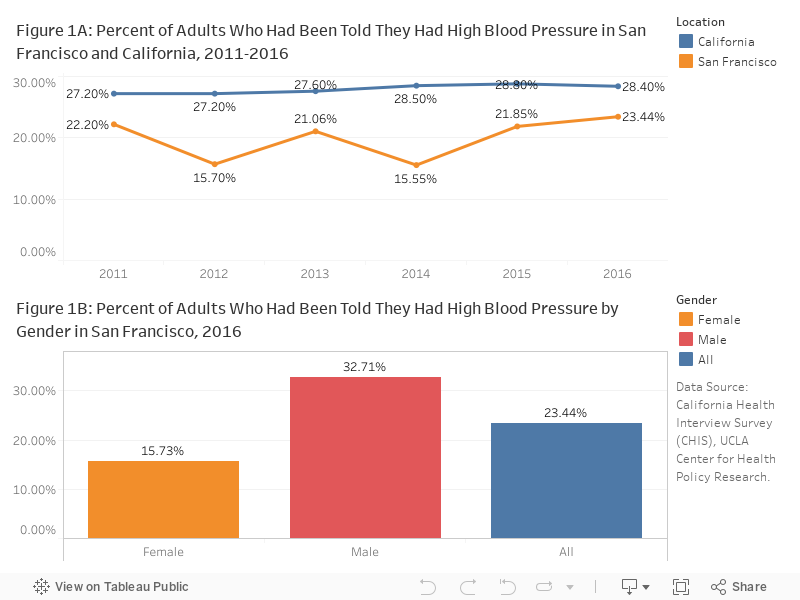
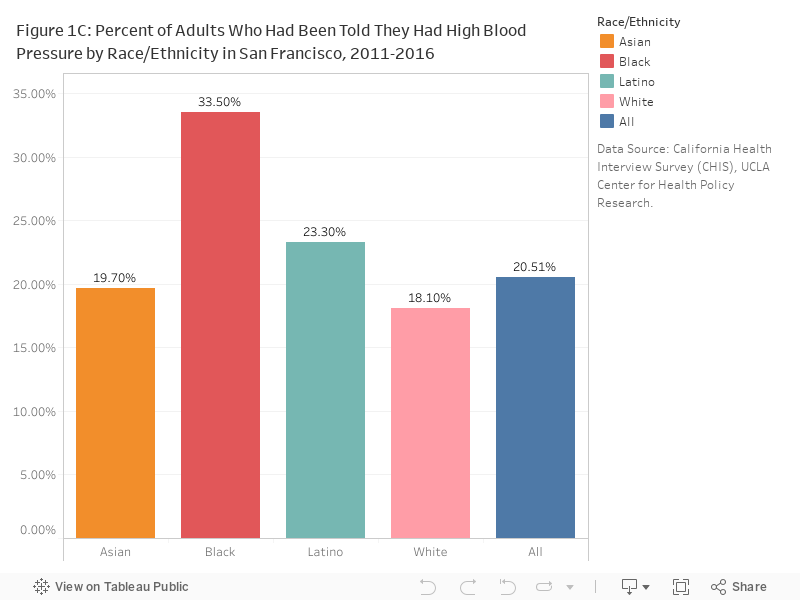
High blood pressure/Hypertension:In 2016, 23.4% of adults living in San Francisco had been told that they had high blood pressure, compared to 28.4% of adults in all of California (Figure 1A). The percent of males (32.7%) with high blood pressure was much higher than females (15.7%) in 2016 (Figure 1B) and Black/African Americans (33.5%) had the highest percent in 2011-16 (Figure 1C).
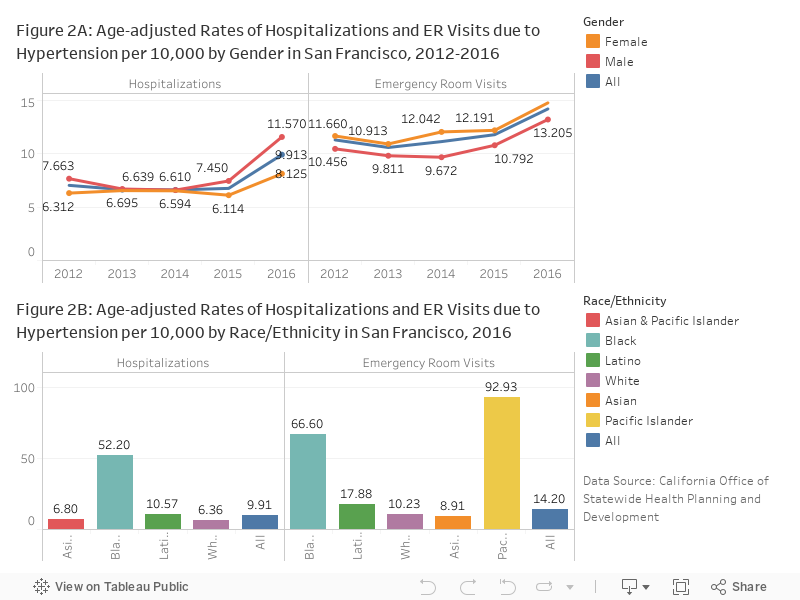
Hospitalization rates due to hypertension, a major contributor to cardiovascular disease, including stroke and chronic heart failure, in San Francisco were fairly stable from 2012 to 2015 but increased by almost 50% in 2016 (9.91 per 10,000 residents), and the emergency room visit rates have been increasing as well (Figure 2A). The rates for Black/African Americans were 3-5 times higher than other races; Pacific islanders had the highest emergency room visit rate (92.9 per 10,000 residents) among all races in 2016 (Figure 2B).
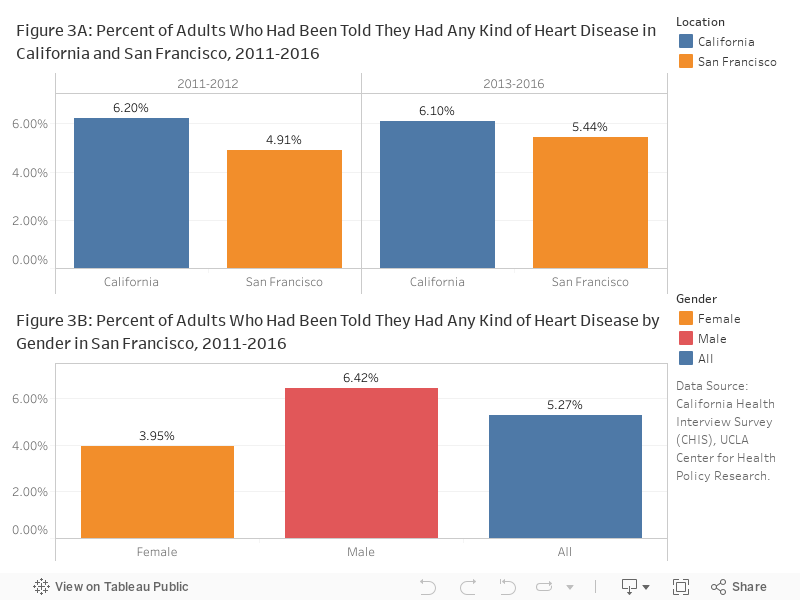
Heart disease/Heart failure: Overall, 5.4% of the adults in San Francisco had been told they had any kind of heart disease in 2013-2016, which is slightly lower than 6.1% for California (Figure 3A). Generally, male adults were more likely to have any kind of heart disease than female adults (Figure 3B).
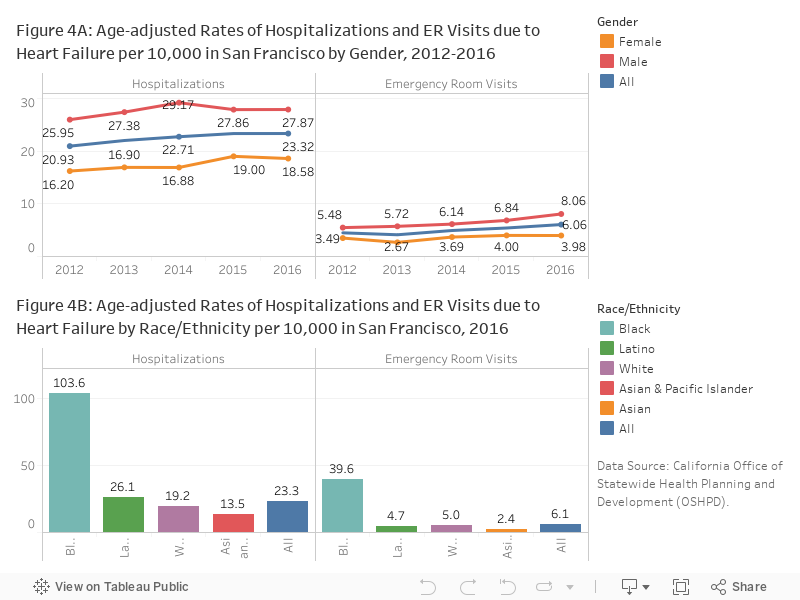
While the hospitalization and emergency room visit rates due to heart failure in San Francisco were fairly stable (Figure 4A), the rates for Black/African American were the highest among all races (Figure 4B).
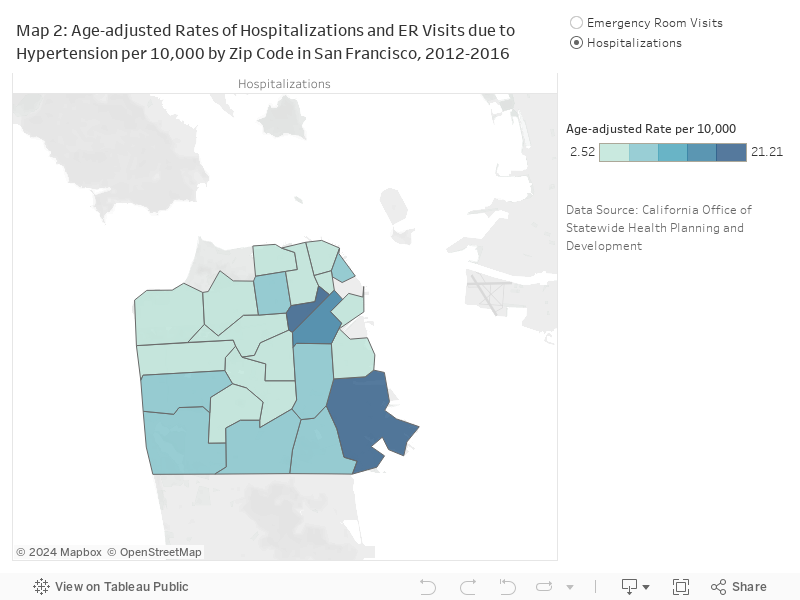
The impact of cardiovascular disease, in terms of hospitalizations and emergency room visits, in San Francisco was higher among residents in the southeast half of San Francisco and among those who live in households earning less than 300 percent of the Federal Poverty Level (FPL). Residents living in the zip codes 94102, 94103, 94124, and 94130 had the highest hospitalization and emergency room visit rates for hypertension and chronic heart failure (Map 2 and Map 4).

Stroke: In 2015, 3.6% of the 69,947 Medicare beneficiaries were treated for stroke in San Francisco. The rate is very close to the rate for California and is ranked the 26th highest county in the state.
CHIS: California Health Interview Survey (CHIS), UCLA Center for Health Policy Research.
Medicare Chronic Conditions Dashboard: http://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Dashboard/Chronic-Conditions-County/CC_County_Dashboard.html
OSHPD: Office of Statewide Health Planning and Development (OSHPD).
Hospitalizations and Emergency Room Visits:
Hospitalization and Emergency Room visit rates measure the number of admissions or visits, not the number of residents who are hospitalized. Admissions records may include multiple admissions by the same person.
In October 2015, the diagnosis coding standard for Hospitalizations and Emergency Room visits was changed from ICD-9 to ICD-10. Caution should be used in comparing data using the two different standards.
Hypertension: Agency for Healthcare Research and Quality’s Clinical Classification Software versions 2015 (ICD-9) and 2017 (ICD-10 ) were used to identify hospitalizations with a primary diagnosis of hypertension.
Heart Failure: ICD-9 and ICD-10 codes for heart failure were adapted from the PQI 08: Heart Failure Admission Rate (September 2017) and PQI 08 :Heart Failure Admission Rate (March 2015) technical specifications published by the Agency for Healthcare Research and Quality. The case definition used here varies from that in the PQI 08 in that records indicating cardiac procedures were not excluded. A medical visit was determined to be primarily due to heart failure if the primary diagnosis field contained the identified ICD-9-CM (discharges prior to October 2015) or ICD-10 (October 2015 and later) codes.
Population estimates for rates:
Standard Population for age adjustment:
Statistical instability: Statistically unstable estimates are not shown in this document. Statistical instability may arise from:
Statistical instability indicates a lack of confidence in the ability of an estimate to accurately and reliably represent the population. Due to statistical instability, estimates are not available for all age, gender, ethnicity, or other groups.
[1] American Heart Association. What is cardiovascular disease. http://www.heart.org/HEARTORG/Caregiver/Resources/ WhatisCardiovascularDisease/What-is-Cardiovascular-Disease_UCM_301852_Article.jsp, 2017.
[2] American Heart Association. What is heart disease and stroke. 2015. http://www.heart.org/idc/groups/heart-public/@wcm/@hcm/documents/downloadable/ucm_300313.pdf.
[3] Healthy People 2020. Heart disease and stroke. http://www.healthypeople.gov/2020/topics-objectives/topic/heart-disease-and-stroke, 2017.
[4] Centers for Disease Control, Prevention (CDC, et al. Vital signs: avoidable deaths from heart disease, stroke, and hypertensive disease-united states, 2001-2010. MMWR. Morbidity and mortality weekly report, 62(35):721, 2013.
[5] Lung National Heart and Blood Institute. What is metabolic syndrome. https://www.nhlbi.nih.gov/health/health-topics/topics/ms, 2016.
[6] American Heart Association. Why metabolic syndrome matters. http://www.heart.org/HEARTORG/Conditions/More/MetabolicSyndrome/Why-Metabolic-Syndrome-Matters_UCM_301922_Article.jsp#.WdVf4FtSzW4, 2016.
[7] American Heart Association. Cardiovascular disease and diabetes. http://www.heart.org/HEARTORG/Conditions/More/Diabetes/WhyDiabetesMatters/Cardiovascular-Disease-Diabetes_UCM_313865_Article.jsp#.WLchClXyuUk, 2015. Accessed March 1, 2017.
[8] American Heart Association. Facts: Bridging the gap, cvd health disparities. 2012.
https://www.heart.org/idc/groups/heart-public/@wcm/@hcm/@ml/documents/downloadable/ucm_429240.pdf.
[9] Donald Lloyd-Jones, Robert Adams, Mercedes Carnethon, Giovanni De Simone, T Bruce Ferguson, Katherine Flegal, Earl Ford, Karen Furie, Alan Go, Kurt Greenlund, Nancy Haase, Susan Hailpern, Michael Ho, Virginia Howard, Brett Kissela, Steven Kittner, Daniel Lackland, Lynda Lisabeth, Ariane Marelli, Mary McDermott, James Meigs, Dariush Mozaffarian, Graham Nichol, Christopher O’Donnell, Veronique Roger, Wayne Rosamond, Ralph Sacco, Paul Sorlie, Randall Stafford, Julia Steinberger, Thomas Thom, Sylvia Wasserthiel-Smoller, Nathan Wong, Judith Wylie-Rosett, Yuling Hong, American Heart Association Statistics Committee, and Stroke Statistics Subcommittee. Heart disease and stroke statistics–2009 update: a report from the american heart association statistics committee and stroke statistics subcommittee. Circulation, 119:e21–181, January 2009.
[10] Centers for Disease Control and Prevention (CDC). Disparities in premature deaths from heart disease–50 states and the district of columbia, 2001. MMWR. Morbidity and mortality weekly report, 53:121–125, February 2004.
[11] J Adam Leigh, Manrique Alvarez, and Carlos J Rodriguez. Ethnic minorities and coronary heart disease: an update and future directions. Current atherosclerosis reports, 18:9, February 2016.
[12] Harvard Health Publishing. Race and ethnicity; clues to your heart disease risk. https://www.health.harvard.edu/heart-health/race-and-ethnicity-clues-to-your-heart-disease-risk, 2015.
[13] LaPrincess C Brewer and Lisa A Cooper. Race, discrimination, and cardiovascular disease. Virtual Mentor, 16(6):455, 2014.
[14] Garth Graham. Disparities in cardiovascular disease risk in the united states. Current cardiology reviews, 11:238–245, 2015.
[15] American Heart Association. Asian & pacific islanders and cardiovascular diseases. https://www.heart.org/idc/groups/heart-public/@wcm/@sop/@smd/documents/downloadable/ucm_319570.pdf, 2013.
