Variables
- General Health Status among Adults
- Disability Status
- Physical or Mental Impairment Preventing Work among Adults
Quality of life is a concept that includes the subjective evaluation of positive and negative aspects of life [1]. The quality of life aspects which affect health or the determinants of health are referred to as health-related quality of life (HRQoL) [2]. HRQoL focuses on the impact health status has on quality of life and is a multidimensional concept including physical, mental, emotional, and social functioning [3]. At the level of the individual, perceptions of physical and mental health and their correlated health risks and conditions, functional status, social support, and socio economic status affect HRQoL. At the community level, factors affecting HRQoL include community level resources, conditions, policies and practices that influence the population’s health perceptions and functional status [2].
Wellbeing is a concept related to HRQOL. It is described by the Centers for Disease Control and Prevention as the presence of positive emotions, absence of negative emotions, general fulfillment, and life satisfaction [4]. People generally achieve life satisfaction through access to basic needs (food, shelter, income), while emotional fulfillment comes from having meaningful relationships. Additional information on community participation is included in the Civic Participation section of this assessment.
According to the World Health Organization, health is “a state of complete physical, mental and social wellbeing and not merely an absence of disease and infirmity [5]. HRQoL provides a comprehensive view of health and is related to both self-reported chronic diseases and their risk factors [2]. In fact, self-assessed health status is a more powerful predictor of morbidity and mortality than many objective measures of health [6, 7].
While the traditional view of prevention emphasizes avoiding illness and risk, promoting wellbeing focuses on disease resistance, resilience, and self-management therefore enhancing protective factors and conditions that promote health.[4] Higher levels of well-being are associated with decreased risk of disease, illness, and injury; better immune functioning; speedier recovery; and increased longevity.[8, 9, 10, 11, 12] Although heritable factors play a role in wellbeing, environmental factors are at least as important.[13, 14, 15, 16]
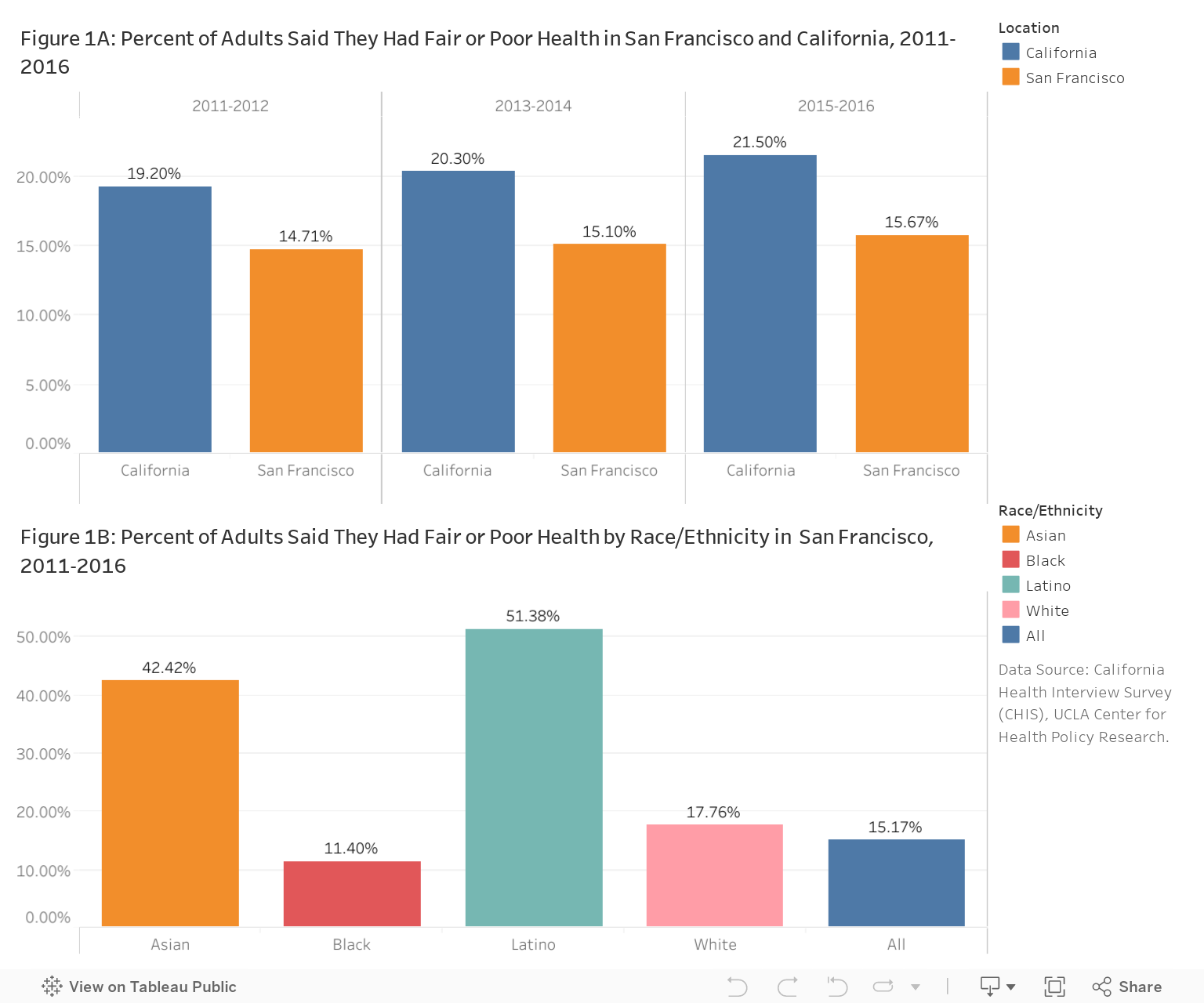
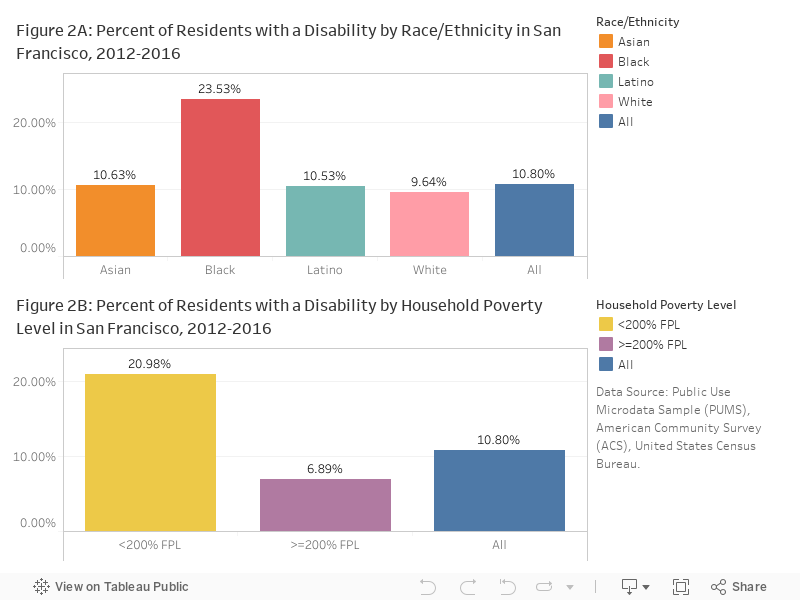
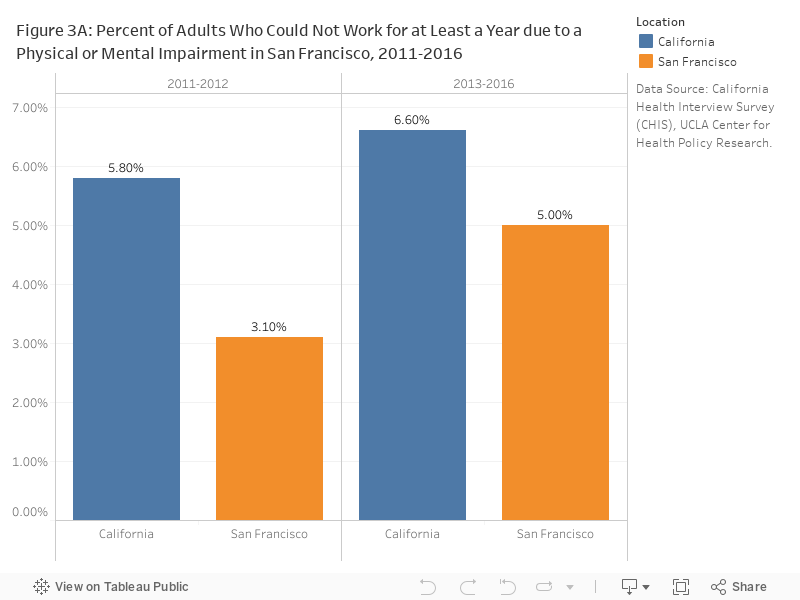
Overall, San Franciscans have health and well-being as good as or better than that Californians overall. In 2016, 15.67% of residents reported having fair or poor health (Figure 1A) and 10.8% reported having a disability in 2012-2016 (Figure 2A). Of adults 18 to 64 years of age, 5% were unable to work for at least one year due to a physical or mental impairment (Figure 3A).
Self-rated health status varies by ethnicity. Latino and Asian residents were more likely to report poor or fair health than were Whites (Figure 1B); Black/African American residents were more likely to have a disability (Figure 2B).
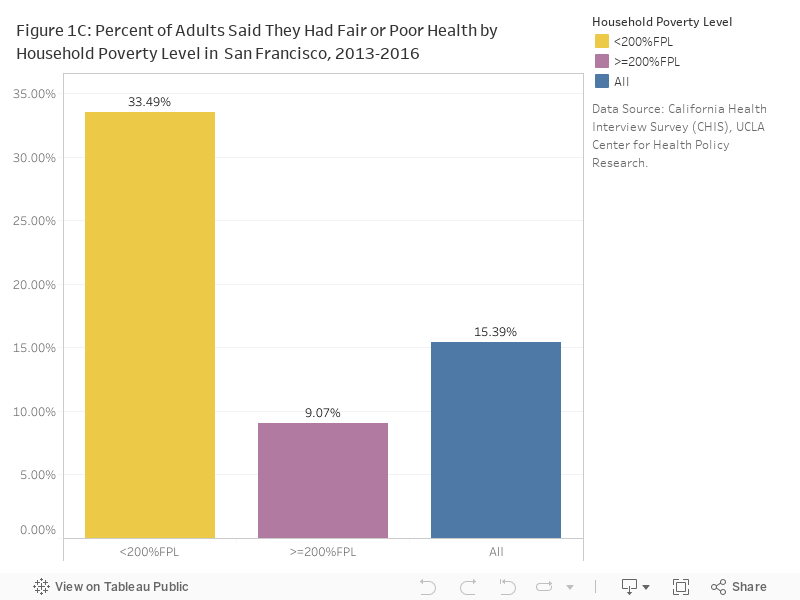
Financial well-being is closely associated with health status and disability; those living in households earning less than 200 percent of the federal poverty level were 3.5 times more likely to report fair or poor health and disability than those with higher household incomes in 2013-2016 (Figure 1C, 2C).
CHIS California Health Interview Survey (CHIS), UCLA Center for Health Policy Research.
PUMS, ACS Public Use Microdata Sample (PUMS), American Community Survey (ACS), United States Census Bureau.
Self-reported health status: CHIS asked participants to describe their health as excellent, very good, good, fair, or poor. The data tables in this report combine percentages from excellent, very good, and good and contrast them to percentages from fair and poor.
Physical and or mental impairment preventing work: This question was only asked of respondents of presumed working age (ages 18 to 64).
Statistical instability: Statistically unstable estimates are not shown in this document. Statistical instability may arise from:
…few respondents to a survey,
…small population sizes, or
…small numbers of affected individuals.
Statistical instability indicates a lack of confidence in an estimates ability to accurately and reliably represent the population. Due to statistical instability, estimates are not available for all age, gender, ethnicity, or other groups.
[1] The WHOQOL Group. The world health organization quality of life assessment (whoqol): development and general psychometric properties. Social science & medicine, 46(12):1569–1585, 1998.
[2] Centers for Disease Control and Prevention. Measuring healthy days: Population assessment of health-related quality of life. Atlanta: CDC, pages 4–6, 2000.
[3] Healthy People 2020. Health-related quality of life and well-being. https://www.healthypeople.gov/2020/topics-objectives/topic/health-related-quality-of-life-well-being, 2017. Accessed March 15, 2017.
[4] Centers for Disease Control and Prevention. Health related quality of life: Well-being concepts. https://www.cdc.gov/hrqol/wellbeing.htm, 2016. Accessed March 15, 2017.
[5] Preamble to the Constitution of the World Health Organization as adopted by the International Health Conference, number 2. Official Records of the World Health Organization, 1946. Accessed March 15, 2017.
[6] Karen B DeSalvo, Nicole Bloser, Kristi Reynolds, Jiang He, and Paul Muntner. Mortality prediction with a single general self-rated health question. a meta-analysis. Journal of general internal medicine, 21:267–275, March 2006.
[7] Kelli L Dominick, Frank M Ahern, Carol H Gold, and Debra A Heller. Relationship of health-related quality of life to health care utilization and mortality among older adults. Aging clinical and experimental research, 14:499–508, December 2002.
[8] Barbara L. Fredrickson and Robert W Levenson. Positive emotions speed recovery from the cardiovascular sequelae of negative emotions. Cognition & emotion, 12(2):191–220, 1998.
[9] E Diener. Biswas–diener, r.(2008). Happiness: unlocking the mysteries of psychological wealth, 86.
[10] G V Ostir, K S Markides, S A Black, and J S Goodwin. Emotional well-being predicts subsequent functional independence and survival. Journal of the American Geriatrics Society, 48:473–478, May 2000.
[11] G V Ostir, K S Markides, M K Peek, and J S Goodwin. The association between emotional well-being and the incidence of stroke in older adults. Psychosomatic medicine, 63:210–215, 2001.
[12] Sarah D Pressman and Sheldon Cohen. Does positive affect influence health? Psychological bulletin, 131:925–971, November 2005.
[13] Bruno S Frey and Alois Stutzer. Happiness and economics: How the economy and institutions affect human well-being. Princeton University Press, 2010.
[14] Ed Diener. Well-being for public policy. Oxford University Press, USA, 2009.
[15] David Lykken and Auke Tellegen. Happiness is a stochastic prhenomenon. Psychological Sciences, 7(3):186–189, 1996.
[16] Ed Diener, Richard E Lucas, and Christie Napa Scollon. Beyond the hedonic treadmill: revising the adaptation theory of well-being. The American psychologist, 61:305–314, 2006.
