Variables
- INTENTION TO EXCLUSIVELY BREASTFEED
- INITIATION OF EXCLUSIVE BREASTFEEDING IN-HOSPITAL
- EXCLUSIVE BREASTFEEDING AT 3 MONTHS
Breast milk is the optimal source of nutrition for most infants. The World Health Organization and American Academy of Pediatrics (AAP) recommend exclusive breastfeeding for about 6 months, with continuation of breastfeeding for 1 year or longer, as mutually beneficial for the mother and infant [1,2]. Exclusive breastfeeding is defined as the infant receiving only breast milk either at the breast or via other feeding methods, and no other liquids or solids with the exception of drops or syrups consisting of vitamins, mineral supplements, or medicines.
The federal initiative, Healthy People 2020, identifies exclusive breastfeeding as a national public health priority, and aims to increase breastfeeding rates such that 46.2 percent of women in the United States exclusively breastfeed for 3 months and 25.5 percent of women exclusively breastfeed for 6 months by 2020 [3]. Compared with other countries, the United States ranks poorly with respect to exclusive breastfeeding. The United States ranks 64th out of 84 countries [4].
Breastfeeding is determined by various factors, including social norms in the community [5], breastfeeding support services available at local delivery hospitals [6-8], workplace policies and practices [9], and local socio-economic conditions [10].
Social marketing and public education about breastfeeding may increase visibility of the topic, promote positive beliefs about breastfeeding, and help mothers and families understand the risks of not breastfeeding [11]. Exposure to positive messages and images about breastfeeding can help make breastfeeding seem normal, feasible, acceptable and expected in the community. In turn, this can make the goal of 6 months of exclusive breastfeeding seem attainable and increase pregnant women’s intention to exclusively breastfeed before birth [12, 13]. Women’s decision-making processes are highly influenced by their social networks [14]. These networks can either be barriers or points of encouragement for breastfeeding.
The initiation of exclusive breastfeeding, at delivery, in hospital, is critical to establish the breast milk supply and increase the likelihood of breastfeeding success and continuation for 6 months [15]. Hospitals that have the Baby-Friendly designation have trained staff and protocol designed to support the initiation of exclusive breastfeeding [16]. Optimally, hospitals will have enough International Board Certified Lactation Consultants (IBCLC) on staff to offer breastfeeding education, support services, and telephone follow-up to inpatients and outpatients. One full-time IBCLC is required for every 783 in-patient mother/baby couplets. One full-time IBCLC is required for every 1292 breastfeeding couplets discharged. One full-time IBCLC is required to provide telephone follow-up for 3915 infants discharged [17].
Workplace lactation support, programs and policies, increase breastfeeding duration [9, 18]. In the U.S, almost 55 percent of women with children under 3 years of age are employed outside the home. Re-integration into the workplace is associated with decreased duration of exclusive breastfeeding [19].
Socioeconomic factors, including race, age, education, income and immigration status, influence breastfeeding initiation, duration, and exclusivity [20]. Neighborhood deprivation is associated with reduced odds of breastfeeding initiation, duration, and exclusivity [21]. Health equity efforts to remove systemic barriers to breastfeeding for women across all social categories and groups are vital to improving breastfeeding rates.
Breastfeeding is associated with health benefits for both the mother and infant. Mothers who do not breastfeed are at higher risk of breast cancer, diabetes mellitus, hyperlipidemia, hypertension, myocardial infarction, obesity, and ovarian cancer [22]. Breastfeeding reduces risk of pediatric infections, such as ear infections and pneumonia, immune disorders, and death in the first year of life [22]. Breastfeeding promotes infant brain development and is associated with improved intelligence by about 2 IQ points [23]. Breastfeeding is consistently associated with a modest reduction in the risk of later overweight and obesity in childhood and adulthood [24]. Breastfeeding has dose-dependent effects, such that both the duration and exclusivity of breastfeeding are associated with positive health benefits [25]. Annually, in the US, billions of dollars could be saved by reducing hypertension and heart attacks, and more than 4,000 infant deaths could be prevented, if 90 percent of U.S. mothers were able to breastfeed for one year after every birth [22].
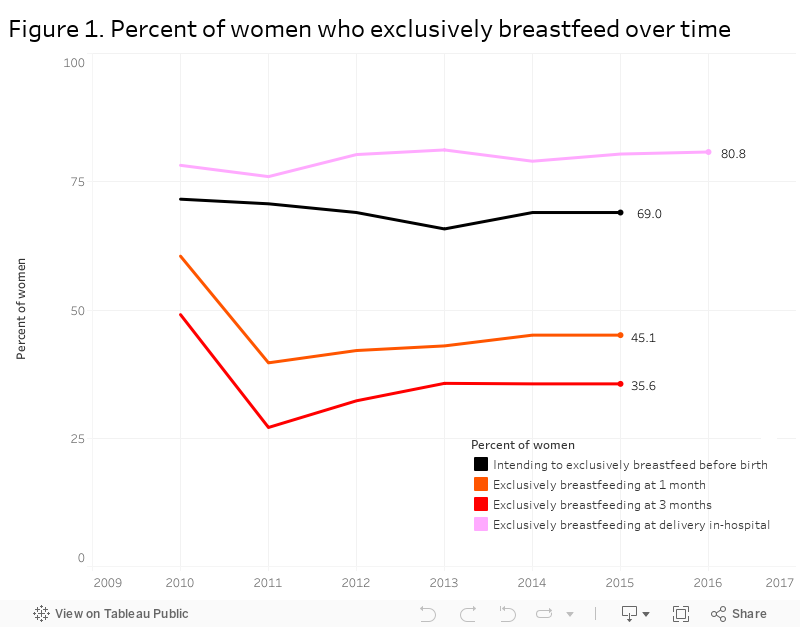
The majority of women in San Francisco do not exclusively breastfeed for longer than one month (see Figure 1). Citywide, between 2010-2015, there were no significant changes in exclusive breastfeeding rates. In 2014–15, only 69 percent of San Francisco women intended to exclusively breastfeed their infant while pregnant. At delivery, in hospital, 81 percent of women initiated exclusive breastfeeding. At 1 month after delivery, 45 percent of women exclusively breastfed. At 3 months after delivery, 36 percent of women exclusively breastfed.
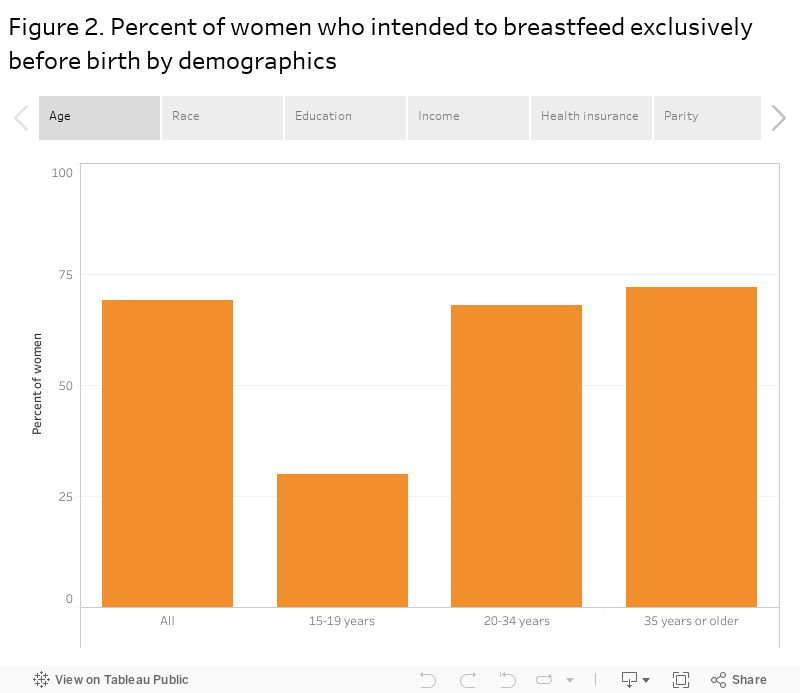
In San Francisco, intention to breastfeed exclusively varies by maternal age, race-ethnicity, education, income, health insurance, and parity (see Figure 2). In 2013-2015, only 30 percent of teens planned to breastfeed exclusively before birth whereas 72 percent of women age 35 or older planned to do so. About 60 percent of Asian/Pacific Islander, Black/African American and Hispanic women intended to breastfeed exclusively compared to 86 percent of White women. An estimated 38 percent of women with a high school degree or GED intended to breastfeed compared to 79 percent of women with a college degree. About half of women with an income below 200 percent of the Federal Poverty Level or public health insurance intended to breastfeed exclusively vs three quarters of women with a higher income or private health insurance. First-time mothers were more likely to intend to breastfeed exclusively than women with two or more children.
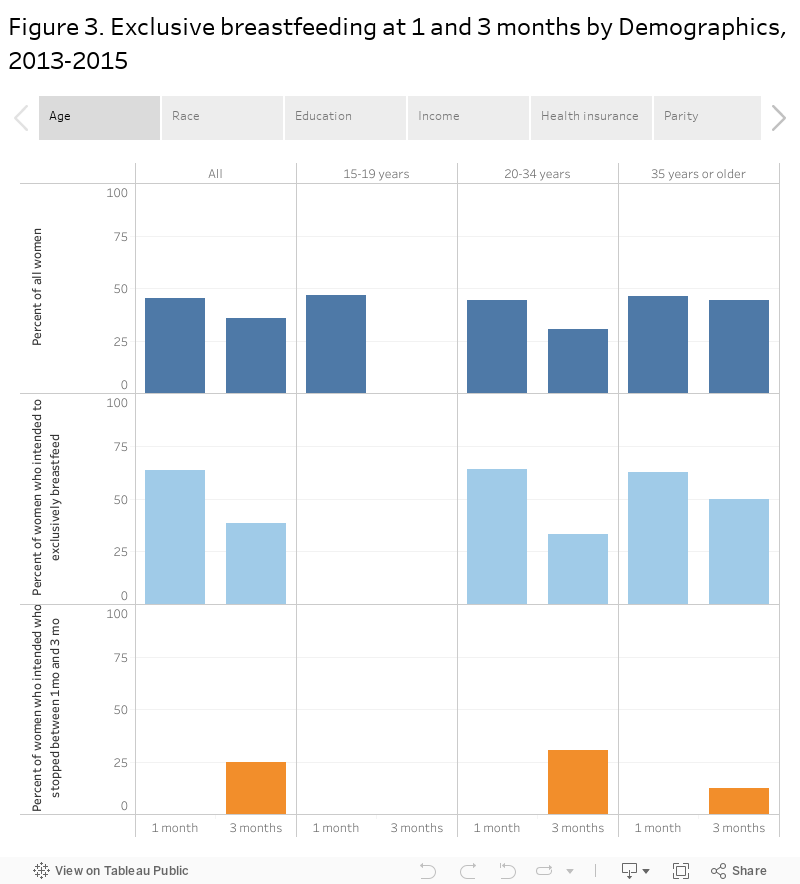
In San Francisco, consistent with variation in intention to exclusively breastfeed, rates of exclusive breastfeeding at 1 month and 3 months varied by mother’s age, race-ethnicity, education, income level, and parity (see Figure 3). While the number of teens who breastfed exclusively at 3 months was too small to estimate (fewer than 5 teens or large standard error), 44 percent of women age 35 or older exclusively breastfed their infants. Under 30 percent of Asian/Pacific Islander and Hispanic women exclusively breastfed at 3 months, compared to 50 percent of White women. The proportion of women with a college degree who exclusively breastfed at 3 months was about triple that of women with less than a high school degree and double that of women with some college coursework but no completed degree. Almost half of women with an income over 200 percent of the Federal Poverty Level exclusively breastfed their infant at 3 months, compared to about 15 percent of women with lower income.
Among women who intended to exclusively breastfeed before birth, the rate of exclusive breastfeeding at 1 month did not differ markedly between groups. Rates were not significantly higher for White vs. Black women, higher income vs lower income, or women with private vs public health insurance. However, after 1 month, rates of exclusive breastfeeding dropped significantly faster for younger, non-White, and lower income groups than for older, White, and higher income groups. The proportion of women with an income below 100 percent of the Federal Poverty Level, who intended to exclusively breastfeed before birth and did so for the 1st month, decreased by 67 percent between 1 and 3 months postpartum. The corresponding decrease among women with an income above 200 percent of the Federal Poverty Level was 30 percent. The same magnitude of difference was seen by type of health insurance. The proportion of women with Medi-cal insurance, who intended to exclusively breastfeed before birth and who did so for the 1st month, decreased by 60 percent between 1 month and 3 months postpartum. On the other hand, the corresponding decrease among women with private health insurance was 30 percent.
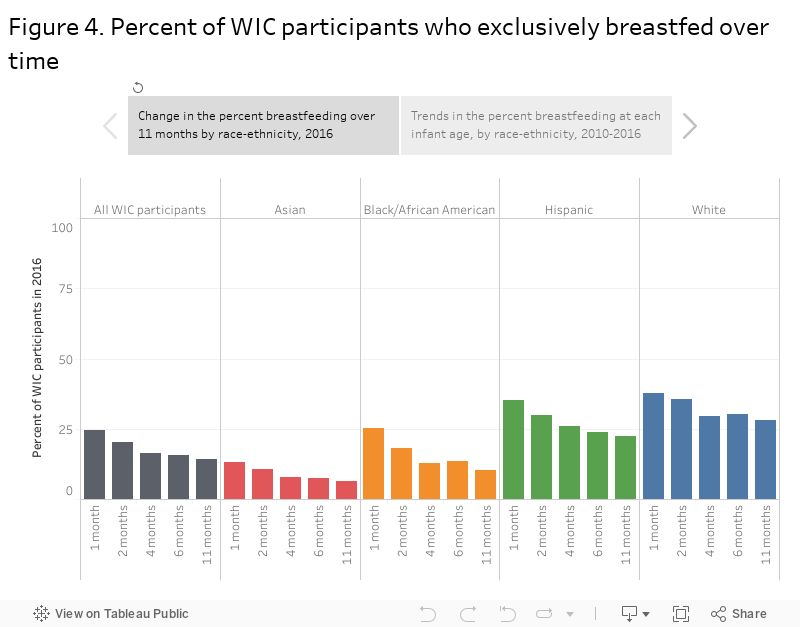
Data from the Women Infants and Children (WIC) program, for participants served in San Francisco over a period of 11 months, further suggest that, within low-income groups, rates of exclusive breastfeeding initiation and duration vary by race-ethnicity (see Figure 4).
Trend data from the WIC program in San Francisco, over the past 5 years, suggest some stabilization or improvement in exclusive breastfeeding rates between 2-4 months for low-income women who self-reported Asian, Black/African American, unspecified race, multiple race or hispanic race-ethnicity, beginning in 2015.
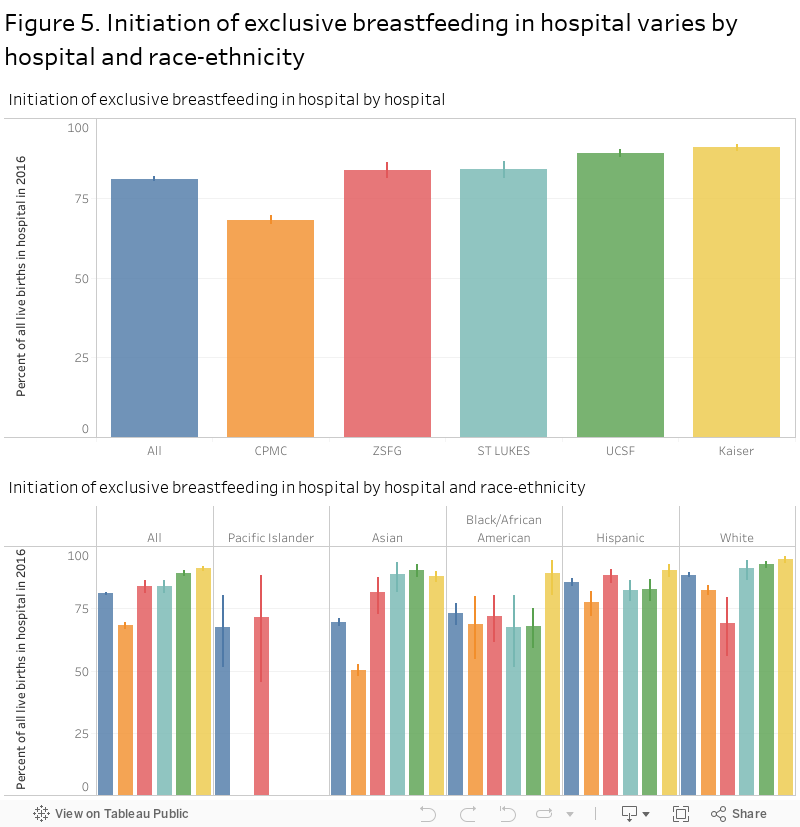
In San Francisco, in 2016, initiation of exclusive breastfeeding at birth varied by hospital (see Figure 5). Only 1 in 5 San Francisco hospitals was Baby-Friendly. Fear of infants becoming dehydrated or hypoglycemic, desire to provide “just one bottle” to help the mother rest, lack of clinician knowledge about breastfeeding, minimal chart documentation about breastfeeding, lack of time to educate new mothers, not placing babies skin-to-skin, extended separation of infants from mothers for routine nursing and medical tasks, use of pacifiers, and free samples of infant formula are noted barriers for local hospital staff to support exclusive breastfeeding [5].
The hospital-specific rates of exclusive breastfeeding initiation varied by race-ethnicity, suggesting need for tailoring of services to support all population groups. The proportion of births covered by Medi-Cal or other public insurance varies by hospital. According to 2016 birth records, 17 percent, 92 percent, 51 percent, 17 percent and 0 percent of the births at CPMC, ZSFG, St Lukes, UCSF and Kaiser were covered by public insurance, respectively.
Lack of hospital outpatient breastfeeding support services is a barrier for exclusive breastfeeding after the delivery, especially for families with Medi-Cal or other public health insurance or coverage. Currently, at ZSFG hospital, where over 90 percent of births are covered by Medi-Cal or other public insurance, there is no dedicated outpatient IBCLC [Personal communication, Teresa Chan, Nutritionist City & County of San Francisco Department of Public Health]. The Peer Counseling Program, designed to support Medi-Cal or WIC-eligible women, only has capacity to serve 128 to 192 breastfeeding women per year. In 2016, there were 2,182 births covered by Medi-Cal or other public insurance in San Francisco.
Lack of breastfeeding friendly infant/child care facilities is also a barrier to breastfeeding exclusivity and duration [Personal communication Grace Yee, WIC Breastfeeding Promotion Coordinator].
To promote a positive image of breastfeeding in public spaces and to celebrate World Breastfeeding Week, San Francisco Department of Public Health Lactation Collaborative organized a month-long photo exhibition at the San Francisco City Hall in August 2017 and 2018. Pictures in 2017 included mothers’ breastfeeding their infants, from eight weeks to almost 2 years old, while sitting on park benches and in grassy areas. Pictures in 2018 included mothers breastfeeding their infants throughout urban San Francisco public spaces from local parks to bus stops.
The collaborative also organized a breastfeeding photo contest for mothers that live and work in San Francisco. Submitted photos were used to create a calendar and distributed to Health Care Provider as a reminder to support breastfeeding families.
WIC and the San Francisco Public Health Lactation Support Collaborative are actively working to support all 5 San Francisco delivery hospitals to adopt breastfeeding friendly policies and practices. The collaborative is also working with primary care clinics to establish outpatient clinical lactation services and support, and increase referral to WIC, Nurse Home Visiting Program, and Black Infant Health Program for prenatal and postpartum education and support for breastfeeding. Some hospitals, WIC, La Leche League and the Homeless Prenatal program offer breastfeeding hotlines/warm lines and mother-to-mother support. WIC, and The Homeless Prenatal Program offers free support groups (https://www.sfhealthnetwork.org/breastfeeding-support/) in different languages to all MediCal or MediCal eligible mothers in San Francisco.
Starting January 1st 2018, San Francisco passed the Lactation in the Workplace ordinance that requires all San Francisco employers regardless of their size to have a policy regarding lactation in the workplace that specifies a process by which an employee requests lactation accommodation and defines minimum standards for lactation accommodation spaces. The policy also requires newly constructed or renovated buildings to include lactation spaces. The San Francisco’s Healthy Mothers Workplace Coalition (through an intensive community engagement process) has developed a workplace tool to assess policies related to parental leave, lactation accommodation, and work-family balance. The tool assesses policies using three levels: bronze (meets requirements), silver (exceeds requirements), and gold (sets a gold standard). The Coalition has given 182 Healthy Mothers Workplace Awards of Excellence to 91 unique employers over the last five years, positively impacting more than 61,000 employees. For further information, please visit: https://legalaidatwork.org/our-programs/healthy-mothers-workplace-coalition-2/
The San Francisco Department of Public Health (www.sfdph.org/breastfeedingatwork ) in partnership with the Office of Labor Standard Enforcement (https://sfgov.org/olse/lactation-workplace) is developing sample policies, best practice guidelines, examples of breastfeeding rooms, employer and employee education materials in multiple languages to especially help small business employing low wage workers in the City.
Local efforts aim to reduce breastfeeding disparities by improving access to breastfeeding services including education and support to priority groups such as African American, Asian/ Pacific Islander, migrant women as well as those who are on Medi-Cal, affected by poverty, unstable housing, nutrition and food insecurity.
For further information about efforts to promote breastfeeding in San Francisco, please visit: http://sfbreastfeeding.org/
and https://www.sfhealthnetwork.org/sfbreastfeeds/
California Department of Public Health, Newborn Screening Program. In-Hospital Breastfeeding Initiation Data.
California Department of Public Health (2018) Maternal and Infant Health Assessment (MIHA) Survey County and Regional Data Snapshots for Subgroups, 2013-2015.
San Francisco Department of Public Health, WIC Program.
Citywide breastfeeding rates were estimated using data from the MIHA survey. The MIHA survey includes only English or Spanish speaking women, and may exclude vulnerable groups, such as housing insecure women who could not be reached, or women who were unable to participate in the written survey. Regarding breastfeeding intention, MIHA survey participants were asked: ‘Before you delivered your baby, how did you plan to feed him or her when he or she was born? (I planned to breastfeed only, I planned to use formula only, I planned to breastfeed and use formula, I was not sure how I would feed my baby)’. Regarding breastfeeding initiation, participants were asked: ‘Has your new baby ever been breastfed or fed breast milk? (yes or no)’. Regarding exclusive breastfeeding in hospital, participants were asked: ‘At the hospital, was your baby fed anything other than breast milk? (yes, no, I don’t know)’. Regarding exclusive breastfeeding at 1 and 3 months, participants were asked: ‘When your baby was one month old, what were you feeding him or her?’ and ‘When your baby was 3 months old what were you feeding him or her?’ (Check all that apply. Breast milk, formula, other liquids, food)’. Breastfeeding estimates were generated for each year and population sub-groups, without adjustment for differences in age or other factors.
Breastfeeding estimates for WIC program participants were determined based on the type of WIC package selected by the participant, which is not the same as self-reported breastfeeding intention or behavior. For further information about WIC packages, please visit: https://www.fns.usda.gov/wic/wic-food-packages.
Information about in-hospital breastfeeding initiation is not available by age of mother or SES variables, such as income. Data quality may vary depending on the timing of the data collection relative to hospital discharge.
[1] WHO. Breastfeeding. http://www.who.int/topics/breastfeeding/en
[2] AAP Policy Statement. Breastfeeding and Use of Human Milk. Pediatrics. 2012. http://pediatrics.aappublications.org/content/early/2012/02/22/peds.2011-3552
[3] https://www.healthypeople.gov/2020/topics-objectives/topic/maternal-infant-and-child-health/objectives
[4] International Baby Food Action Network (2016). Has your nation done enough to bridge the gaps?
[5] Rossman B. Breastfeeding peer counselors in the United States: helping to build a culture and tradition of breastfeeding. J Midwifery Women’s Health. 2007;52(6):631-637. https://www.ncbi.nlm.nih.gov/pubmed/17984001
[6] Vasquez M & Berg O. The Baby-Friendly journey in a US public hospital. J Perinat Neonatal Nurs 2012; 26(1):37-46.
[7] Lee J. Supporting Breastfeeding Moms at Work: How a Doctor’s Note Can Make the Difference. Breastfeed Med. 2017 Oct;12(8):470-472. doi: 10.1089/bfm.2017.0107. Epub 2017 Aug 17.
[8] DiGirolamo AM, Grummer-Strawn LM, Fein SB. Do perceived attitudes of physicians and hospital staff affect breastfeeding decisions? Birth. 2003;30(2):94–100.
[9] Dinour LM, Szaro JM. Employer-Based Programs to Support Breastfeeding Among Working Mothers: A Systematic Review. Breastfeed Med. 2017 Apr;12:131-141. doi: 10.1089/bfm.2016.0182. Epub 2017 Mar 1. https://www.ncbi.nlm.nih.gov/pubmed/28394659
[10] Mercier RJ, Burcher TA, Horowitz R, Wolf A Differences in Breastfeeding Among Medicaid and Commercially Insured Patients: A Retrospective Cohort Study. Breastfeed Med. 2018 May;13(4):286-291. doi: 10.1089/bfm.2017.0228. Epub 2018 Mar 13. https://www.ncbi.nlm.nih.gov/pubmed/29634340
[11] Schmidt M. Social marketing and breastfeeding: a literature review. Glob J Health Sci. 2013 Feb 8;5(3):82-94. doi: 10.5539/gjhs.v5n3p82. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4776800/pdf/GJHS-5-82.pdf
[12] Stuebe AM, Bonuck K. What predicts intent to breastfeed exclusively? Breastfeeding knowledge, attitudes, and beliefs in a diverse urban population. Breastfeed Med. 2011 Dec;6(6):413-20. doi: 10.1089/bfm.2010.0088. Epub 2011 Feb 22.
[13] Raissian KM, Su JH. The best of intentions: Prenatal breastfeeding intentions and infant health.
SSM Popul Health. 2018 Jun 18;5:86-100. doi: 10.1016/j.ssmph.2018.05.002. eCollection 2018 Aug.
[14] Renfrew MJ, McCormick FM, Wade A, Quinn B, Dowswell T. Support for healthy breastfeeding mothers with healthy term babies. Published in final edited form as: Cochrane Database Syst Rev. 2012 May 16; 5: CD001141. Published online 2012 May 16. doi: 10.1002/14651858.CD001141.pub4. Update in: Cochrane Database Syst Rev. 2017 Feb; 2017(2): 10.1002/14651858.CD001141.pub5.
[15] Office of the Surgeon General (US). “The Surgeon General’s Call to Action to Support Breastfeeding.” Advances in Pediatrics., U.S. National Library of Medicine, 1 Jan. 1970, www.ncbi.nlm.nih.gov/books/NBK52682/.
[16] Baby-Friendly USA. The gold standard of care. https://www.babyfriendlyusa.org/
[17] Mannel R, Mannel RS. Staffing for hospital lactation programs: recommendations from a tertiary care teaching hospital. J Hum Lact. 2006 Nov;22(4):409-17. www.ncbi.nlm.nih.gov/pubmed/17062786.
[18] Kim JH, Shin JC, Donovan SM. Effectiveness of Workplace Lactation Interventions on Breastfeeding Outcomes in the United States: An Updated Systematic Review. J Hum Lact. 2018 Jun 1:890334418765464. doi: 10.1177/0890334418765464. [Epub ahead of print]
[19] Fernández-Cañadas Morillo A, Durán Duque M, Hernández López AB, Muriel Miguel C, Martínez Rodríguez B, Oscoz Prim A, Pérez Riveiro P, Salcedo Mariña A, Royuela Vicente A, Casillas Santana ML, Marín Gabriel MA. A Comparison of Factors Associated with Cessation of Exclusive Breastfeeding at 3 and 6 Months. Breastfeed Med. 2017 Sep;12(7):430-435. doi: 10.1089/bfm.2017.0045. Epub 2017 Aug 8.
[20] Stough CO, Khalsa AS, Nabors LA, Merianos AL, Peugh J. Predictors of Exclusive Breastfeeding for 6 Months in a National Sample of US Children. Am J Health Promot. 2018 Jan 1:890117118774208. doi: 10.1177/0890117118774208. [Epub ahead of print] https://www.ncbi.nlm.nih.gov/pubmed/28787188
[21] Peregrino AB, Watt RG, Heilmann A, Jivraj S. Breastfeeding practices in the United Kingdom: Is the neighbourhood context important? Matern Child Nutr. 2018 Jun 11:e12626. doi: 10.1111/mcn.12626. [Epub ahead of print]
[22] Schwarz EB, Nothnagle M.The maternal health benefits of breastfeeding. Am Fam Physician. 2015 May 1;91(9):603-4.
[23] Rouw E, von Gartzen A, Weißenborn A. [The importance of breastfeeding for the infant].[Article in German]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2018 Aug;61(8):945-951. doi: 10.1007/s00103-018-2773-4.
[24] Patro-Gołąb B, Zalewski BM, Kołodziej M, Kouwenhoven S, Poston L, Godfrey KM, Koletzko B, van Goudoever JB, Szajewska H. Nutritional interventions or exposures in infants and children aged up to 3 years and their effects on subsequent risk of overweight, obesity and body fat: a systematic review of systematic reviews. Obes Rev. 2016 Dec;17(12):1245-1257. doi: 10.1111/obr.12476. Epub 2016 Oct 17.
[25] Furman L. Breastfeeding: What Do We Know, and Where Do We Go From Here? Pediatrics 2017; 139(4) e201701050. http://pediatrics.aappublications.org/content/pediatrics/139/4/e20170150.full.pdf
